Abstract
Objective: Smartphones, now ubiquitous across the globe, have the potential to contribute to behavioral addiction. Among the psychological concerns linked to such addictions are depression and anxiety. This study aimed to investigate potential associations between smartphone addiction and symptoms of depression and anxiety in a sample of young adults.
Methods: This descriptive, cross-sectional study was conducted over a two-month period among 512 university students. Participants completed a questionnaire comprising sociodemographic information and smartphone usage patterns, along with the Smartphone Addiction Scale–Short Version (SAS-SV), Beck Depression Inventory (BDI), and Beck Anxiety Inventory (BAI). Group comparisons were performed using the Kruskal–Wallis and Mann–Whitney U tests. Spearman and Pearson correlation coefficients were used to assess the strength and direction of associations.
Results: The study population consisted of young adults with a mean age of 20.45 ± 1.95 years.A statistically significant relationship was found between depression-based on cut-off values-and smartphone addiction (p=0.001). Moreover, weak but statistically significant positive associations were observed between smartphone addiction and both depression (r=0.232, p=0.001) and anxiety (r=0.209, p=0.001). Participants who self-identified as smartphone addicts reported significantly higher SAS-SV scores compared to those who were unsure or did not consider themselves addicted (p=0.001).
Conclusions: The findings demonstrate a significant association between smartphone addiction and symptoms of depression and anxiety. Given that individuals perceiving themselves as addicted exhibited notably higher addiction scores, self-perception may serve as a useful indicator in preventive mental health approaches—particularly within the context of primary care.
Keywords: Smartphone addiction, internet addiction disorder, depression, anxiety, mental health
Introduction
In recent years, smartphones have become an integral part of daily life for most people worldwide. According to data from the Turkish Statistical Institute (2024), 86.2% of children aged 11 to 15 use smartphones.[1] The increasing exposure to enjoyable digital content and the early age at which smartphones are adopted raise concerns regarding their potential to foster behavioral addiction.
Growing interest among physicians in behavioral addictions has highlighted both the potential negative implications (e.g., stigmatization) and positive outcomes (e.g., preventive interventions, early identification, and evidence-based treatments) associated with diagnosing such conditions.[2] The American Psychiatric Association (APA) refers to behavioral addictions in the DSM-5-TR (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision), listing gambling disorder as a recognized behavioral addiction and identifying internet gaming disorder as a condition warranting further study.[3] Similarly, the World Health Organization's ICD-11 (International Classification of Diseases, 11th Revision) categorizes "disorders due to addictive behaviors", which includes both gambling and gaming disorders, each further classified by online or offline predominance.[4,5]
Although standardized diagnostic criteria for smartphone addiction have not yet been established, a growing body of research has positioned it as a form of behavioral addiction that is increasingly attracting clinical attention.[6-8] A comprehensive meta-analysis of over 500 studies across 64 countries, encompassing more than two million participants, estimated the global prevalence of smartphone addiction at 26.99%.[7]
Furthermore, studies have shown that behavioral addictions may co-occur with other mental health conditions, particularly anxiety and depression, emphasizing their significance not only as independent psychiatric disorders but also as part of broader comorbid profiles.[6,8]
The aim of this study was to investigate the prevalence of smartphone addiction among young adults, to identify potential contributing factors, and to examine associations between smartphone addiction and symptoms of anxiety and depression.
Materials and Methods
This descriptive, cross-sectional study was conducted among volunteer students from the Faculty of Health Sciences (Department of Nursing) and the Faculty of Medicine at Ankara Yıldırım Beyazıt University, all of whom were at least 18 years old and reported no history of psychiatric disorders. Following the provision of informed verbal and written consent, 558 questionnaires were distributed. Of these, 35 were excluded due to incomplete responses and 11 due to a self-reported history of psychiatric disorders, the final sample consisted of 512 participants.
The data collection tool consisted of a structured questionnaire assessing sociodemographic characteristics and smartphone use patterns, alongside the Smartphone Addiction Scale-Short Version (SAS-SV)[9,10], the Beck Depression Inventory (BDI)[11,12] and the Beck Anxiety Inventory (BAI).[13,14]
Smartphone Addiction Scale – Short Version
Originally developed by Kwon et al. as a 33-item scale to assess smartphone addiction[15], the SAS was later condensed into a 10-item version to enhance usability.[9] The items are categorized as follows: daily life disturbance (items 1–3), withdrawal (items 4–7), and one item each on virtual relationship orientation, overuse, and tolerance (items 8–10). In the Korean sample, cut-off scores were reported as 31 for males and 33 for females.[9] A Turkish validation and reliability study was conducted by Noyan et al. in 2015[10]; however, no established cut-off score exists for the Turkish version.
Beck depression inventory
The BDI, developed by Beck et al. in 1961[11], is a widely used 21-item scale for assessing depressive symptoms and severity. Validity and reliability in the Turkish context were confirmed by Hisli (1989), and it was stated that scores of 17 and above among Turkish university students indicate a risk group for depression.[12]
Beck anxiety inventory
The BAI, created by Beck et al. in 1988[13], includes 21 items measuring anxiety symptoms experienced in the preceding week. The Turkish validation study was conducted by Ulusoy in 1993.[14]
Data collection took place over two months. Questionnaires and scales were distributed during class breaks, and participants completed them independently. Researchers were available for clarification as needed.
All responses were digitally recorded. Statistical analysis was performed using IBM SPSS version 24.0. Descriptive statistics were expressed as means ± standard deviations or percentages. Statistical significance was defined as p< 0.05. Non-parametric group comparisons were made using the Kruskal–Wallis test and, if significant, followed by the Mann–Whitney U test for pairwise analysis. The strength and nature of the association were assessed using Spearman or Pearson correlation analysis, depending on data distribution.
Results
Participant characteristics
A total of 512 students participated in the study: 24.6% (n=126) were male and 75.4% (n=386) were female. The mean age was 20.45 ± 1.95 years, ranging from 18 to 30. Among participants, 45.5% (n=233) were enrolled in the Faculty of Medicine and 54.5% (n=279) in the Faculty of Health Sciences (Department of Nursing).
Smartphone usage characteristics
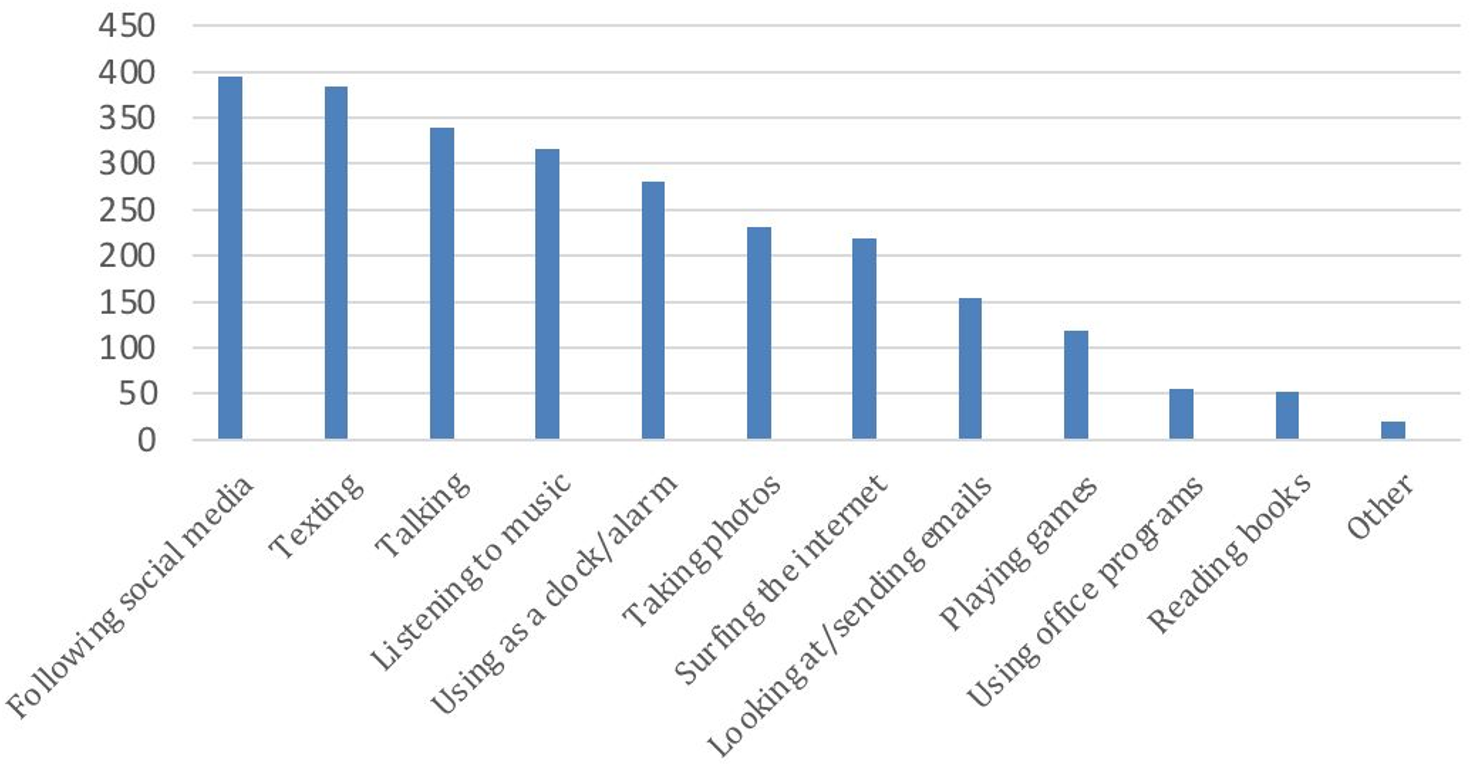
The vast majority of students (99.2%, n=508) owned a smartphone. On average, participants had been using smartphones for 7.35 ± 2.85 years and reported an average daily usage of 4.44 ± 2.72 hours (range: 0–16 hours). Figure 1 presents the distribution of smartphone usage purposes, where participants could select multiple options.
Smartphone addiction scores and influencing variables
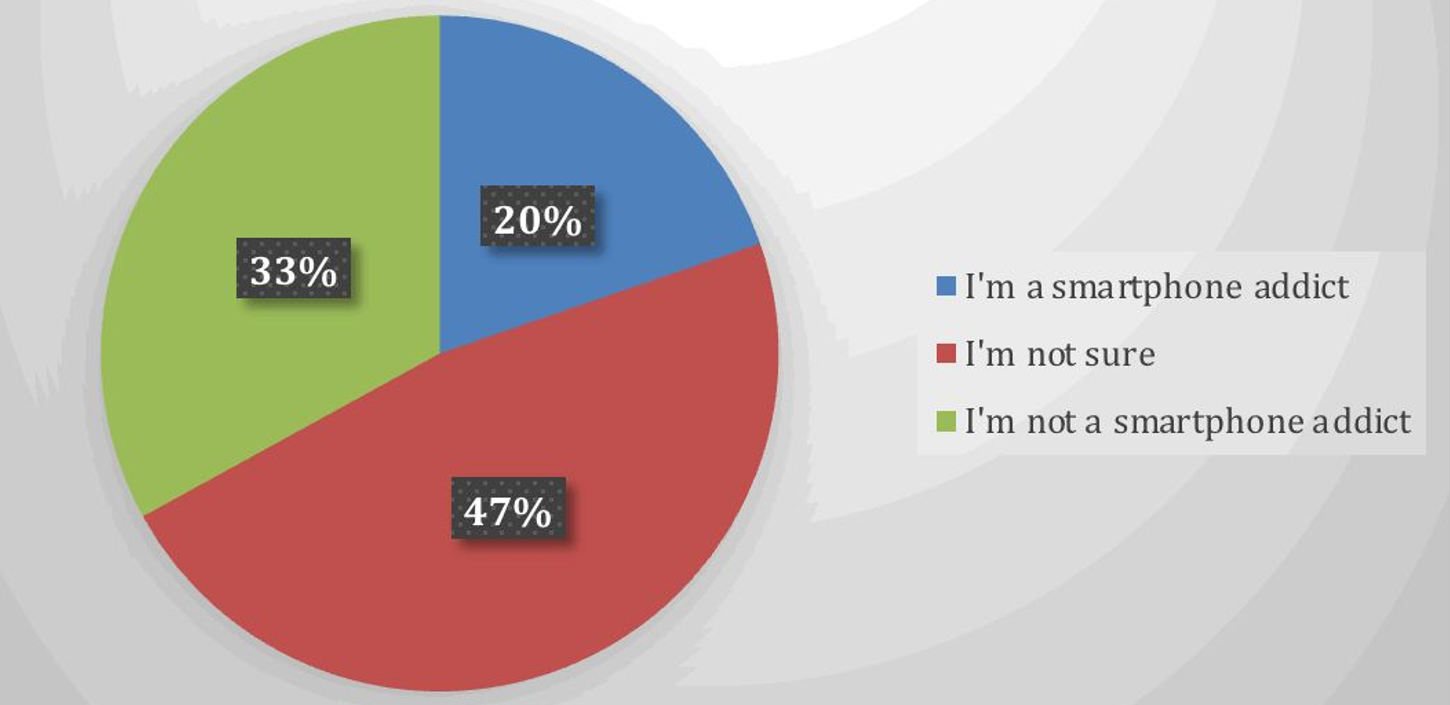
SAS-SV scores ranged from 10 to 60, with a mean of 28.69 ± 10.19. Since the Turkish version lacks an established cut-off score, prevalence rates could not be determined. When asked, 20% of participants self-identified as smartphone addicts (Figure 2).
Statistical analysis revealed that female participants had significantly higher SAS-SV scores than males (p=0.004). No significant associations were observed between smartphone addiction and participants' age (p=0.27) (Table 1).
| Mann-Whitney U test and Kruskal-Wallis Analysis were used. | |||
| Table 1. Comparison of SAS-SV scores by gender and age | |||
|
|
|
||
| Gender |
|
|
|
|
|
|
||
| Age (years) |
|
|
|
|
|
|
||
|
|
|
||
|
|
|
||
|
|
|
||
|
|
|
||
|
|
|
||
|
|
|
||
|
|
|
||
|
|
|
||
|
|
|
||
|
|
|
||
Participants who used their smartphones for social media, photography, or listening to music had significantly higher SAS-SV scores (all p< 0.01; Table 2).
| Mann-Whitney U test was used. | |||
| Table 2. Relationship between smartphone usage purpose and SAS-SV scores | |||
| Usage Purpose |
|
|
|
| Social Media |
|
|
|
|
|
|
||
| Taking Photos |
|
|
|
|
|
|
||
| Listening to Music |
|
|
|
|
|
|
||
There was a highly significant relationship between daily smartphone usage duration and SAS-SV scores (p=0.001); addiction scores increased with duration of use. A Kruskal–Wallis test was conducted to examine differences in SAS-SV scores across four usage duration groups. The results indicated a statistically significant difference in SAS-SV scores among the groups (p<0.001). Subsequent pairwise Mann–Whitney U tests revealed a clear pattern of increasing SAS-SV scores with longer usage duration (Table 3).
| Different letters (a, b, c, d) indicate statistically significant differences between groups (p<0.001). Kruskal-Wallis Analysis was used. Pairwise comparisons were conducted using Mann-Whitney U tests with Bonferroni correction. | ||
| Table 3. Association between daily smartphone usage duration and SAS-SV scores | ||
| Usage Duration (hours) |
|
|
| Less than 1 |
|
|
| 1-2 |
|
|
| 3-4 |
|
|
| More than 4 |
|
|
Participants who self-identified as smartphone addicts had significantly higher SAS-SV scores than those who were unsure or disagreed. Pairwise comparisons were conducted using Mann–Whitney U tests with Bonferroni correction. All pairwise post-hoc comparisons between groups were statistically significant. Overall, these results suggest a stepwise increase in SAS-SV scores across the three categories, with Addict participants showing the highest levels of smartphone addiction symptoms, followed by Not Sure, and then Not Addict participants (Table 4).
| Different letters (a, b, c) indicate statistically significant differences between groups (p<0.001). Kruskal-Wallis Analysis was used. Pairwise comparisons were conducted using Mann–Whitney U tests with Bonferroni correction. | ||
| Table 4. Relationship between self-perceived smartphone addiction and SAS-SV scores | ||
| Self-Perception |
|
|
| Addict |
|
|
| Not Sure |
|
|
| Not Addicted |
|
|
Smartphone addiction, depression and anxiety sympthoms levels
BDI analysis showed that 18.2% (n=93) of participants scored above the cut-off point of 17. Students with scores above 17 had significantly higher SAS-SV scores than those below the cut-off (p=0.001).
Spearman correlation analysis indicated a weak but statistically significant positive relationship between smartphone addiction and both depression and anxiety sympthoms levels (Table 5).
| Spearman Correlation Analysis was used. | ||||
| Table 5. Associations between smartphone addiction and depression and anxiety sympthoms levels | ||||
|
|
|
|||
|
Smartphone Addiction |
|
|
|
|
|
|
|
|
|
|
Discussion
In our study, SAS-SV scores were positively and significantly correlated with BDI and BAI scores. This aligns with previous research suggesting associations between smartphone use and mental health outcomes.
Although the term smartphone addiction is commonly used, alternative expressions such as smartphone dependency[16], excessive smartphone use[17], problematic smartphone use[18-20], nomophobia (No Mobile Phone PhoBIA)[21] appear frequently in the literature. Despite terminological variations, a systematic review of 27 studies has confirmed a link between smartphone addiction and mental health issues.[6] The present findings, emphasizing a significant relationship between smartphone addiction and depressive and anxiety symptoms, align with previous results.[6]
A large-scale study from Korea involving 4,854 adults reported similar findings: both internet and smartphone addiction were associated with higher levels of depression and anxiety sympthoms.[22] Interestingly, the association was stronger for smartphone addiction than for internet addiction[22], suggesting that smartphone addiction may constitute a distinct behavioral concern—despite its absence from formal diagnostic manuals such as the DSM-5-TR[3] and ICD-11[4].
Our results are also in agreement with prior cross-sectional studies showing a linear association between SAS-SV and BDI scores[23], and with other findings linking smartphone use with elevated depression and trait anxiety scores based on the PUMP (Problematic Use of Mobile Phones) scale[20]. In a multicenter study involving 1,236 university students, each unit increase in smartphone addiction score was associated with a 7% rise in anxiety among males and 9% among females.[16] Similarly, data from postgraduate students across 187 universities worldwide revealed a significant association between smartphone addiction and Major Depressive Disorder (MDD).[24] Although these studies used varying terminologies[16,20,23,24], they collectively support the positive association we observed between smartphone addiction and psychological distress. Notably, the cross-sectional nature of these studies (including ours) precludes conclusions about causality.[16,20,23,24]
A longitudinal study from Korea tracking 1,877 adolescents over three years found a bidirectional relationship between smartphone addiction and depressive symptoms, with both intensifying over time.[25] Another Turkish study employing multiple regression analysis also identified depression and anxiety as significant predictors of smartphone addiction.[26] These findings underscore the importance of prospective studies to better understand the causal pathways involved.
In our study, participants who self-identified as smartphone addicts scored significantly higher on the SAS-SV. This suggests that a simple self-report question like "Do you perceive yourself as a smartphone addict?" may offer practical value in screening, especially given the potential psychological comorbidities.[6]
We observed a significant association between smartphone addiction and female gender. This finding is supported by some studies[16,17], but contradicted by others reporting no gender difference[24] or higher addiction levels among males[27]. Such discrepancies may reflect sample characteristics, as in our study, where females represented more than 75% of participants or differing usage patterns, such as males being more vulnerable to gaming- or internet-related addiction.[7]
No significant relationship was found between age and smartphone addiction in our sample. This contrasts with a previous SAS-SV-based study involving adults over 55 years, which reported higher addiction scores among younger users.[23] Our narrower age range may explain this divergence.
Participants who reported using smartphones for social media, photography, or music had significantly higher addiction scores. This is not surprising, as social media addiction alone affects an estimated 17.42% of the global population according to a meta-analysis of over 500 studies.[7] Moreover, a randomized controlled trial in 2022 found that abstaining from social media for just one week resulted in improved well-being and reduced symptoms of depression and anxiety.[28] While photo-taking behavior may be linked to social media use, our findings are supported by previous research associating selfie-taking with problematic smartphone use.[18] The link between music listening and addiction requires further investigation to better understand underlying mechanisms.
Limitations
Due to the cross-sectional design, causal relationships between smartphone addiction and depression or anxiety cannot be established. Moreover, because there is no validated cut-off score for the Turkish version of the SAS-SV[10], we were unable to calculate prevalence rates. Our sample was limited to students from two faculties with a predominantly female composition and a narrow age range, which may limit generalizability and influence gender-related findings.
Conclusions
This study identified a significant association between smartphone addiction and symptom levels of depression and anxiety. Risk factors for higher smartphone addiction scores included female gender, increased daily smartphone usege duration, and usage for social media, photography, or music. Individuals who self-perceived as addicted had significantly higher SAS-SV scores, suggesting that direct questioning may have value in early identification efforts, particularly in primary care and preventive mental health settings. Future research, especially longitudinal studies, is needed to further elucidate these associations.
Ethical approval
Ethics committee approval was obtained from Ankara Yıldırım Beyazıt University Faculty of Medicine Clinical Research Ethics Committee with the decision numbered 293 and dated 21.12.2016.
Source of funding
The authors declare that the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest to disclose.
Acknowledgements
During the preparation and revision of this manuscript, artificial intelligence tools (Microsoft Copilot and ChatGPT) were used solely to improve the clarity, grammar, and academic writing style of the text. No AI tools were used for data analysis, interpretation, generation of scientific content, or drawing conclusions. All content was reviewed and approved by the authors, who take full responsibility for the final version of the manuscript.
References
- Türkiye İstatistik Kurumu. Çocuklarda bilişim teknolojileri kullanım araştırması-2024. 2024. Available at: https://data.tuik.gov.tr/Bulten/Index?p=Cocuklarda-Bilisim-Teknolojileri-Kullanim-Arastirmasi-2024-53638 (Accessed on Dec 28, 2024).
- Petry NM, Zajac K, Ginley MK. behavioral addictions as mental disorders: to be or not to be? Annu Rev Clin Psychol. 2018;14:399-423. https://doi.org/10.1146/annurev-clinpsy-032816-045120
- American Psychiatric Association. DSM-5-TR Classification. Diagnostic and statistical manual of mental disorders. 2022. https://doi.org/10.1176/appi.books.9780890425787
- World Health Organization (WHO). ICD-11 for mortality and morbidity statistics. Available at: https://icd.who.int/browse/2024-01/mms/en#499894965%2Funspecified (Accessed on Dec 28, 2024).
- Brand M, Potenza MN. behavioral addictions in the ıcd-11: an important debate that is anticipated to continue for some time. J Behav Addict. 2023;12(3):585-589. https://doi.org/10.1556/2006.2023.00042
- Ratan ZA, Parrish AM, Zaman SB, Alotaibi MS, Hosseinzadeh H. Smartphone addiction and associated health outcomes in adult populations: a systematic review. Int J Environ Res Public Health. 2021;18(22):12257. https://doi.org/10.3390/ijerph182212257
- Meng SQ, Cheng JL, Li YY, et al. Global prevalence of digital addiction in general population: a systematic review and meta-analysis. Clin Psychol Rev. 2022;92:102128. https://doi.org/10.1016/j.cpr.2022.102128
- Osorio-Molina C, Martos-Cabrera MB, Membrive-Jiménez MJ, et al. Smartphone addiction, risk factors and its adverse effects in nursing students: a systematic review and meta-analysis. Nurse Educ Today. 2021;98:104741. https://doi.org/10.1016/j.nedt.2020.104741
- Kwon M, Kim DJ, Cho H, Yang S. The smartphone addiction scale: development and validation of a short version for adolescents. PLoS One. 2013;8(12):e83558. https://doi.org/10.1371/journal.pone.0083558
- Noyan CO, Enez Darçin A, Nurmedov S, et al. Validity and reliability study of the short form of the smartphone addiction scale in Turkish among university students. Anatolian Journal Of Psychiatry. 2015;16:71-83. https://doi.org/10.5455/apd.176101
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4:561-571. https://doi.org/10.1001/archpsyc.1961.01710120031004
- Hisli N. Validity and reliability of the beck depression inventory for university students. Turkish Journal of Psychology. 1989;7:3-13.
- Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol. 1988;56(6):893-897. https://doi.org/10.1037//0022-006x.56.6.893
- Ulusoy M. Beck anksiyete envanteri-geçerlik ve güvenirlik çalışması. İstanbul: Bakırköy Ruh ve Sinir Hastalıkları Hastanesi; 1993.
- Kwon M, Lee JY, Won WY, et al. Development and validation of a smartphone addiction scale (SAS). PLoS One. 2013;8(2):e56936. https://doi.org/10.1371/journal.pone.0056936
- Lee KE, Kim SH, Ha TY, et al. Dependency on smartphone use and its association with anxiety in Korea. Public Health Rep. 2016;131(3):411-419. https://doi.org/10.1177/003335491613100307
- Tangmunkongvorakul A, Musumari PM, Thongpibul K, et al. Association of excessive smartphone use with psychological well-being among university students in Chiang Mai, Thailand. PLoS One. 2019;14(1):e0210294. https://doi.org/10.1371/journal.pone.0210294
- Richardson M, Hussain Z, Griffiths MD. Problematic smartphone use, nature connectedness, and anxiety. J Behav Addict. 2018;7(1):109-116. https://doi.org/10.1556/2006.7.2018.10
- Elhai JD, Yang H, Fang J, Bai X, Hall BJ. Depression and anxiety symptoms are related to problematic smartphone use severity in Chinese young adults: fear of missing out as a mediator. Addict Behav. 2020;101:105962. https://doi.org/10.1016/j.addbeh.2019.04.020
- El-Sayed Desouky D, Abu-Zaid H. Mobile phone use pattern and addiction in relation to depression and anxiety. East Mediterr Health J. 2020;26(6):692-699. https://doi.org/10.26719/emhj.20.043
- Notara V, Vagka E, Gnardellis C, Lagiou A. The emerging phenomenon of nomophobia in young adults: a systematic review study. Addict Health. 2021;13(2):120-136. https://doi.org/10.22122/ahj.v13i2.309
- Kim YJ, Jang HM, Lee Y, Lee D, Kim DJ. Effects of internet and smartphone addictions on depression and anxiety based on propensity score matching analysis. Int J Environ Res Public Health. 2018;15(5):859. https://doi.org/10.3390/ijerph15050859
- Alhassan AA, Alqadhib EM, Taha NW, Alahmari RA, Salam M, Almutairi AF. The relationship between addiction to smartphone usage and depression among adults: a cross sectional study. BMC Psychiatry. 2018;18(1):148. https://doi.org/10.1186/s12888-018-1745-4
- Alageel AA, Alyahya RA, A Bahatheq Y, et al. Smartphone addiction and associated factors among postgraduate students in an Arabic sample: a cross-sectional study. BMC Psychiatry. 2021;21(1):302. https://doi.org/10.1186/s12888-021-03285-0
- Jun S. The reciprocal longitudinal relationships between mobile phone addiction and depressive symptoms among Korean adolescents. Computers in Human Behavior 2016;58:179-186. https://doi.org/10.1016/j.chb.2015.12.061
- Aker S, Şahin MK, Sezgin S, Oğuz G. Psychosocial factors affecting smartphone addiction in university students. J Addict Nurs. 2017;28(4):215-219. https://doi.org/10.1097/JAN.0000000000000197
- Song A, Song G, Wang H, et al. Prevalence of mobile phone addiction among medical students: a systematic review. Am J Transl Res. 2023;15(5):2985-2998.
- Lambert J, Barnstable G, Minter E, Cooper J, McEwan D. Taking a one-week break from social media ımproves well-being, depression, and anxiety: a randomized controlled trial. Cyberpsychol Behav Soc Netw. 2022;25(5):287-293. https://doi.org/10.1089/cyber.2021.0324
Copyright and license
Copyright © 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.