Abstract
Objective: This study aimed to adapt the Gosnell Pressure Ulcer Risk Assessment Scale into Turkish and to evaluate its linguistic validity, content validity, inter-observer reliability, and construct validity through exploratory and confirmatory factor analyses.
Methods: This methodological study was conducted with 150 patients treated in a palliative care unit over one year. The adaptation process consisted of two stages: linguistic validation and assessment of validity and reliability. Linguistic validity was assessed using the translation-back translation method and expert reviews. Content validity was evaluated using the Lawshe technique with input from five experts from the Department of Family Medicine. Reliability was assessed by measuring inter-observer agreement using the Kappa coefficient, Cramer’s V coefficient, and Spearman correlation analysis. To evaluate construct validity, Exploratory Factor Analysis (EFA) using Principal Component Analysis and Confirmatory Factor Analysis (CFA) using the Diagonally Weighted Least Squares (DWLS) estimation method were conducted.
Results: A total of 150 participants were included, with a mean age of 74.74 years, and 58% were female. The Content Validity Ratio (CVR) for each item was calculated as 1. Regarding reliability, the Kappa coefficient for the Mental Status item was 0.903, and Cramer’s V coefficient was 0.896; for the Continence, Mobility, and Activity items, both the Kappa and Cramer’s V coefficients were 1. For the Nutrition item, the Kappa coefficient was 0.840, and Cramer’s V coefficient was 0.862. A significant and positive correlation was found between the total scores of the two observers (p<0.001). For construct validity, the EFA revealed a single-factor structure explaining 62.039% of the total variance, with a Kaiser-Meyer-Olkin (KMO) value of 0.783 and Bartlett’s test of sphericity being significant (χ²(10)=383.266, p<0.001). The subsequent CFA showed a marginal model fit (χ²/df=5.627), while all factor loadings were statistically significant (p<0.001). The Nutrition item demonstrated a relatively lower loading (0.457), suggesting possible cultural or contextual differences in the Turkish sample.
Conclusion: The Turkish version of the Gosnell Pressure Ulcer Risk Assessment Scale was found to be a valid and reliable tool for use by healthcare professionals in Türkiye. The scale showed acceptable content and construct validity.
Keywords: Pressure ulcer, risk assessment scale, validity, reliability, exploratory factor analysis, confirmatory factor analysis
Introduction
Pressure ulcers are a common and serious complication often resulting from immobility and comorbidities.[1] These ulcers typically develop in areas where bones exert pressure on hard surfaces such as the sacrum, heels, ischium, and trochanter in adults, and the occipital region in children due to factors such as reduced immune response, hormonal changes, and decreased blood flow.[2-6]
As defined in the 2019 Clinical Practice Guideline on the Prevention and Treatment of Pressure Ulcers/Injuries, a pressure ulcer is localized damage to the skin or underlying tissue resulting from sustained pressure, or a combination of pressure and shear forces.[7] This condition places significant financial burdens on healthcare systems and patients, with annual treatment costs reaching $17.8 billion in the United States alone. In Türkiye, around 300,000 patients require pressure ulcer treatment each year, leading to an economic impact of approximately $1.425 billion.[8,9]
The most effective way to mitigate the morbidity, mortality, and financial burden associated with pressure ulcers is prevention, including risk assessment, skin care, use of supportive surfaces, and patient education.[10] Risk assessment scales, such as the Norton, Braden, Gosnell, and Waterlow scales, are widely used to identify patients at risk.[2]
The Norton Scale, developed in 1962, rates five parameters to identify risk, while the Braden Scale includes six subscales and is commonly used with a cut-off score of 16. The Waterlow Scale, based on the Norton Scale, assesses eight parameters, including body mass index and medication use. While the Braden, Norton, and Waterlow scales have undergone Turkish validity and reliability studies, the Gosnell Pressure Ulcer Scale has not yet been validated in Turkish.[2,11-16]
Therefore, the aim of this study is to translate and culturally adapt the Gosnell Pressure Ulcer Scale into Turkish and to evaluate its reliability and validity.
Methods
Type of research
This methodological study aimed to adapt the Gosnell Pressure Ulcer Risk Assessment Scale into Turkish and to evaluate its validity and reliability. The study was conducted in the Palliative Care Unit of Kütahya University of Health Sciences Evliya Çelebi Training and Research Hospital, with data collected between October 2022 and November 2023. Eligible patients participated voluntarily.
Population and sample
For methodological studies, a sample size at least five times greater than the number of scale items is recommended. Thus, with five items on the scale, the minimum required sample size was 25 participants. However, to enhance statistical power, the sample size was increased to 150 patients.
Inclusion criteria
- Voluntary participation
- Aged 18 years or older
- Presence of a pressure ulcer (excluding Stage 4) or absence of pressure ulcer development
- Currently receiving treatment in the palliative care unit
- Hospitalized for more than 14 days
Data collection tools
Data were gathered using a Sociodemographic Questionnaire and the Gosnell Pressure Ulcer Risk Assessment Scale.
- Sociodemographic Form: This form, developed based on the relevant literature, consists of two sections: (1) basic demographics (e.g., age, gender, chronic illness) and (2) pressure ulcer-related data (e.g., stage, location).[7,17-19]
- Gosnell Pressure Ulcer Risk Assessment Scale: Developed by Davina J. Gosnell in 1973 and revised in 1989, this scale comprises five primary items: mental status (5 points), continence, mobility, activity (4 points each), and nutrition (3 points). Additional factors such as vital signs and skin appearance, while included in the assessment, do not affect the total score, which ranges from 5 to 20. Patients scoring 16 or above are considered at high risk for pressure ulcers.[2,17-19]
Language validity study
The scale was translated into Turkish by three independent English-proficient individuals. The Turkish version was then reviewed by a Turkish language expert for accuracy. Following revisions, the scale was back-translated into English. No semantic discrepancies were identified. The final version was confirmed by three academic experts specializing in pressure ulcers.
Validity study of the scale
To assess content validity, the Lawshe method was employed. Five experts evaluated the scale items using a three-point Likert scale:
- The item is essential and must be included.
- The item is useful but may require revision.
- The item is not necessary.
The Content Validity Ratio (CVR) for each item was calculated using the following formula:
CVR=[G / (N / 2)] − 1
Where G is the number of experts rating the item as “essential,” and N is the total number of experts. Items with a CVR of 0 or less were to be removed.[20] Since no items in this study had a CVR value of 0 or less, none were excluded.
Items with a positive CVR were compared to the minimum required CVR value, which was determined to be 0.99 at a significance level of α=0.05 for a panel of 5–7 experts.
Reliability study of the scale
To assess reliability, the scale was administered independently by two observers for each patient. Inter-observer agreement was analyzed using the Kappa coefficient and Cramer’s V.
- A Kappa value between 0.81 and 1.00 indicates “very good agreement,”
- 0.61–0.80 “good agreement,”
- 0.41–0.60 “moderate agreement,”
- 0.21–0.40 “fair agreement,”
- 0–0.20 “poor agreement,”
- <0 “no agreement.”
Cramer's V (υ) ranges from 0 to 1:
- υ=0 indicates no relationship,
- υ=1 indicates perfect relationship,
- υ → 0 indicates a weak relationship,
- υ → 1 indicates a strong relationship.[20]
Data analysis
Statistical analyses were conducted using IBM SPSS Statistics for Windows, Version 29.0 (IBM Corp., Armonk, NY, USA). Normally distributed numerical variables between two groups were analyzed using the Independent Samples t-test. Relationships between non-normally distributed numerical variables were assessed using Spearman's correlation analysis. Inter-observer agreement was evaluated using Kappa coefficients, and Cramer’s V was used to assess the strength of association. The level of statistical significance was set at p<0.05.
In addition, exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were conducted to assess the construct validity of the scale. The EFA was performed using principal component analysis with Varimax rotation, and the suitability of the data for factor analysis was confirmed with the KMO measure and Bartlett’s test. CFA was carried out using the Diagonally Weighted Least Squares (DWLS) method due to the ordinal nature of the data.
Ethical aspect of the research
Ethical approval was obtained from the Non-Interventional Clinical Research Ethics Committee of Kütahya University of Health Sciences, Faculty of Medicine (Approval No.: 2022/09-13, Date: 14.09.2022).
Results
A total of 150 patients were included in the study. The mean age of the participants was 74.7 ± 13.9 years, and 58% were female. Cardiovascular disease was the most prevalent chronic condition, reported by 64% of the patients. Prior to hospitalization, 55.3% of the patients had used air mattresses, and 98% were dependent on diapers. The sociodemographic characteristics of the study population are presented in Table 1.
| *Mean±SD; **Urological diseases, musculoskeletal diseases. | |
| Table 1. Sociodemographic characteristics and comorbidities | |
|
|
|
| Age (years) |
|
| Gender | |
| Female |
|
| Male |
|
| Comorbidities | |
| Cardiovascular Disease |
|
| Neurological Disease |
|
| Diabetes Mellitus |
|
| Malignancy |
|
| Respiratory Diseases |
|
| Renal Diseases |
|
| Liver Diseases |
|
| Other Diseases** |
|
| Use of Air Mattress |
|
The distribution of the patients' nutritional routes is shown in Table 2.
| Table 2. Distribution by nutritional route | |
|
|
|
| Oral |
|
| Percutaneous Endoscopic Gastrostomy |
|
| Nasogastric Tube |
|
| Parenteral |
|
Pressure ulcers were most commonly observed on the sacrum. Notably, 2% of the patients did not develop any pressure ulcers during their hospital stay. The localization of pressure ulcers is detailed in Table 3.
| Table 3. Localization of pressure ulcers | |
|
|
|
| Sacrum |
|
| Spine |
|
| Coccyx |
|
| Right Trochanter |
|
| Right Ischial Tuberosity |
|
| Left Ischial Tuberosity |
|
| Right Lower Leg |
|
| Left Heel |
|
| Right Heel |
|
| Right Scapula |
|
| Right Iliac Crest |
|
| Left Iliac Crest |
|
| Left Knee |
|
| Left Lower Leg |
|
| Right Foot Toes |
|
Validity findings of the scale
The content validity of the Turkish version of the Gosnell Pressure Ulcer Risk Assessment Scale was assessed using the Lawshe method. Five experts evaluated each of the five items, and all items achieved a Content Validity Ratio (CVR) of 1.00, exceeding the minimum acceptable value of 0.99. The Content Validity Index (CVI), calculated as the average of the CVR values, was also above the recommended threshold of 0.67, indicating excellent content validity.
Construct validity was then examined using Exploratory Factor Analysis (EFA). The Kaiser–Meyer–Olkin (KMO) value of 0.783 and Bartlett’s test of sphericity (χ²(10)=383.266, p<0.001) confirmed that the data were suitable for factor analysis. The EFA identified a single-factor structure that explained 62.0% of the total variance, as detailed in Table 4, which presents the factor loadings for each item and supports the unidimensional structure of the scale.
| KMO=0.783, Bartlett’s χ²(10)=383.266, p<0.001 Explained Variance=62.0% |
|
| Table 4. Exploratory factor analysis results for the Gosnell pressure ulcer risk assessment scale | |
| Item |
|
| Mental Status |
|
| Continence |
|
| Mobility |
|
| Activity |
|
| Nutrition |
|
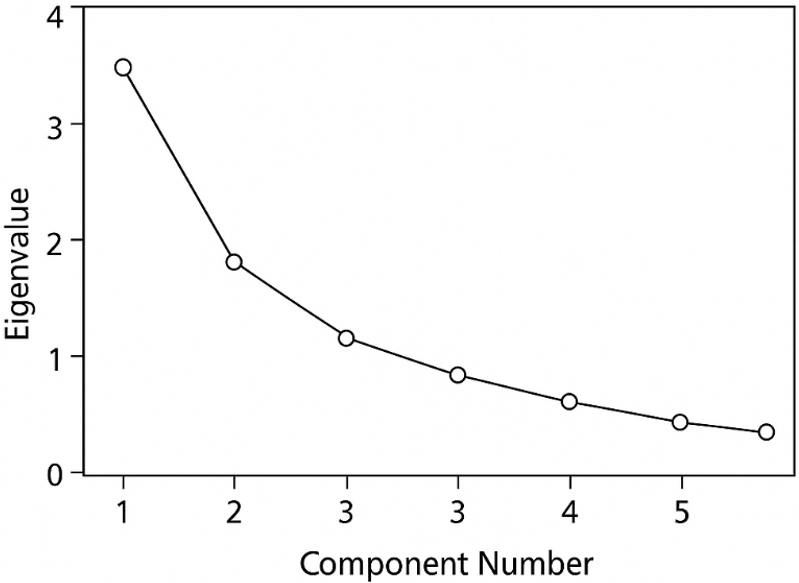
A clear inflection was observed after the first component in the scree plot (Figure 1), confirming that the scale has a unidimensional structure.
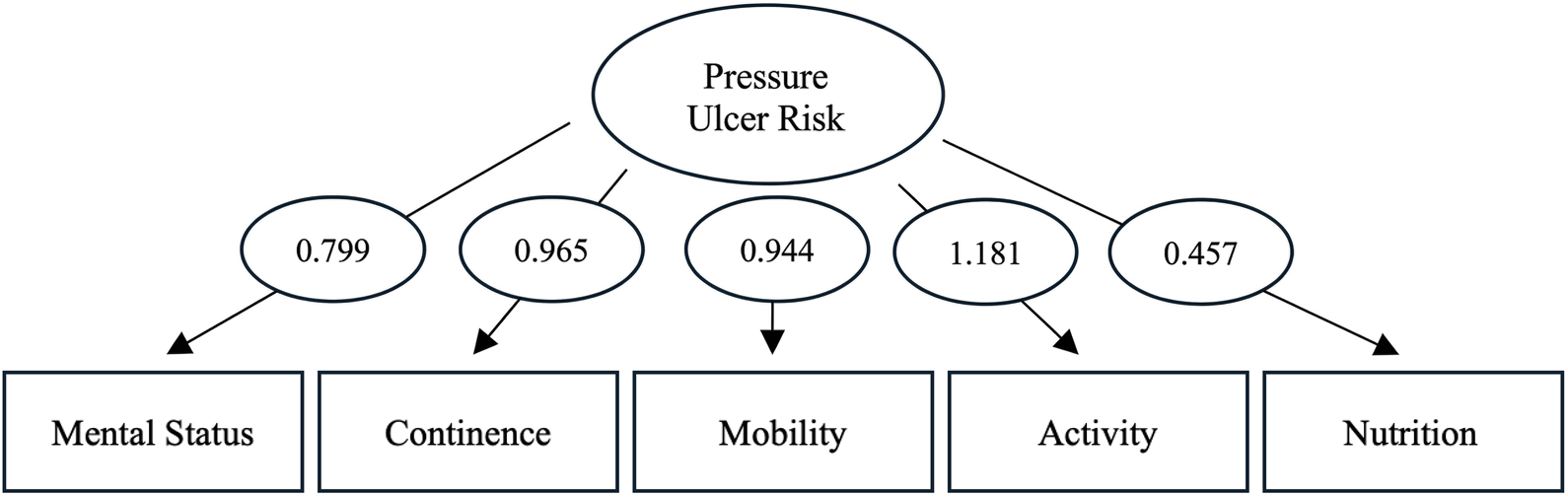
A confirmatory factor analysis (CFA) was conducted to verify the one-factor structure obtained from the EFA. The analysis used the Diagonally Weighted Least Squares (DWLS) estimation method. The model demonstrated acceptable fit (χ²(5)=28.137, p<0.001). All standardized factor loadings were statistically significant (p<0.001) and ranged from 0.457 to 1.181, confirming that all items contributed meaningfully to the latent construct. The model’s path diagram is shown in Figure 2, and detailed loadings and fit indices are presented in Table 5.
| Table 5. Confirmatory factor analysis standardized loadings and fit indices | |
| Item |
|
| Mental Status |
|
| Continence |
|
| Mobility |
|
| Activity |
|
| Nutrition |
|
|
Model Fit Indices: χ²(5)=28.137, p<0.001. Estimation Method: DWLS. |
|
Reliability findings of the scale
The Gosnell Pressure Ulcer Risk Assessment Scale includes five core items: Mental Status, Continence, Mobility, Activity, and Nutrition. Each item is evaluated according to specific response options that reflect the patient’s overall risk profile. The agreement between the two observers for these items was examined, and the results are summarized in Table 6.
| *Chi-square test. | ||||||
| Table 6. Inter-observer agreement for all items and response options of the Gosnell Scale | ||||||
| Item | Response Options |
(n, %) |
(n, %) |
|
|
|
| Mental Status | Alert |
|
|
|
|
|
| Apathetic |
|
|
||||
| Confused |
|
|
||||
| Stuporous |
|
|
||||
| Unconscious |
|
|
||||
| Continence | Fully Controlled |
|
|
|
|
|
| Usually Controlled |
|
|
||||
| Minimally Controlled |
|
|
||||
| Absence of Control |
|
|
||||
| Mobility | Mobile |
|
|
|
|
|
| Slightly Limited |
|
|
||||
| Very Limited |
|
|
||||
| Immobile |
|
|
||||
| Activity | Ambulatory |
|
|
|
|
|
| Walks with Assistance |
|
|
||||
| Chairfast |
|
|
||||
| Bedfast |
|
|
||||
| Nutrition | Good |
|
|
|
|
|
| Fair |
|
|
||||
| Poor |
|
|
||||
The inter-rater reliability analysis revealed a high degree of agreement between observers, as evidenced by Kappa coefficients ranging from 0.840 to 1.000 and strong Cramer’s V associations across all items. Statistical significance was confirmed for all findings (p<0.001, Chi-square test).
The internal consistency of the Turkish version of the Gosnell Pressure Ulcer Risk Assessment Scale was then examined using Cronbach’s alpha. The coefficient for the overall scale was 0.817, reflecting a high level of internal consistency. Item–total correlations ranged from 0.318 to 0.757, showing that all items contributed meaningfully to the overall construct, although the Nutrition item exhibited a relatively lower correlation. The stability of the scale’s internal structure was further supported by the fact that the removal of any item did not notably increase the alpha value, as shown in Table 7.
| Table 7. Item-total correlations and Cronbach’s alpha values for the Turkish version of the Gosnell Scale (n=150) |
||
| Item |
|
|
| Mental Status |
|
|
| Continence |
|
|
| Mobility |
|
|
| Activity |
|
|
| Nutrition |
|
|
| Overall scale (5 items) |
|
|
Correlation analysis of total scores revealed a positive and significant relationship between the scores of the first and second observers (p<0.001). Table 8 presents the correlation analysis of the total scores on the Gosnell scale between observers.
| Spearman correlation analysis between total scores of the two observers. | ||
| Table 8. Correlation of total scores | ||
|
|
|
|
| Spearman’s rho |
|
|
| p-value |
|
|
Discussion
Various methods are employed to assess whether the linguistic validity of a scale accurately reflects the original version. One of the most utilized approaches is the traditional method, which consists of three stages. The first stage involves translating the scale from the source language to the target language, followed by back-translation into the original language. In the final stage, both translations are reviewed by experts and tested on a sample group to ensure clarity and accuracy.[21,22] In our study, the traditional method was adopted to establish linguistic validity. Language experts carefully reviewed each stage, and necessary revisions were made.
To assess the appropriateness, representativeness, and cultural relevance of the scale and its items, content validity was evaluated using expert assessments and the Lawshe method. Five experts rated each item using a three-point scale, and the Content Validity Ratio (CVR) was calculated for each item. Items with positive CVR values were compared to the minimum required CVR values listed in the reference table, based on the number of experts and a significance level of α=0.05. For 5–7 experts, the minimum acceptable CVR value is 0.99. In this study, all items achieved a CVR of 1.00, indicating their appropriateness, and no items were excluded. Subsequently, the Content Validity Index (CVI) for the overall scale was calculated and found to exceed 0.67, which was statistically significant.[20,23]
Beyond content validity, the construct validity of the Turkish version was also evaluated. Exploratory and confirmatory factor analyses were conducted, revealing a strong unidimensional structure. The EFA accounted for over 62% of the total variance, and CFA demonstrated a good model fit with significant factor loadings. These results support the internal structure and cultural adaptability of the scale.
The reliability of a scale can be evaluated using various methods. In this study, inter-observer reliability was assessed to determine the consistency of the Gosnell Pressure Ulcer Risk Assessment Scale. The scale was administered independently by two observers within 24 hours of the patient's admission. The Kappa coefficient was used to evaluate inter-observer agreement, while Cramer’s V coefficient assessed the strength of associations. In addition, the Spearman correlation coefficient was calculated to assess the correlation between the total scores of the two observers. A strong and statistically significant correlation (r=0.987, p<0.001) supports the consistency of the scale when used by different raters.
As shown in the analyses presented in Tables 6 and Table 7, the Kappa coefficient indicated excellent agreement across all items, and Cramer’s V coefficient demonstrated strong associations. Furthermore, Spearman correlation analysis of total scores revealed a positive and statistically significant correlation between the two observers. These findings confirm the reliability of the scale based on the conducted statistical analyses.
Although the Gosnell Pressure Ulcer Risk Assessment Scale has been frequently utilized in clinical settings, its cross-cultural adaptation and validation studies remain limited in the international literature. To the best of our knowledge, the only publication addressing the validity of the Gosnell scale in a non-English context is a Spanish-language study titled “Validación de dos escalas de valoración del riesgo de úlceras por presión: Gosnell y Nova-4,” published in Enfermería Viva in 1999. This prospective study compared the original Gosnell scale with a modified version of the Nova-4 scale in four hospital units, focusing on predictive validity, sensitivity, and specificity.[24] The authors reported that the Gosnell scale demonstrated acceptable predictive value but relatively low specificity, ultimately recommending the alternative scale for routine use.
It is important to note, however, that the aforementioned study did not conduct a formal linguistic adaptation process for the Gosnell scale, nor did it evaluate the instrument using content validity indices or inter-rater reliability statistics. In contrast, the present study represents the first known effort to adapt the Gosnell scale into Turkish through a systematic methodological process, including forward and back translation, expert evaluation using the Lawshe technique, and detailed assessment of inter-observer agreement through the Kappa coefficient and Cramer’s V.
The findings of our study demonstrate that all items on the Turkish version of the scale met the necessary criteria for content validity, and inter-observer agreement across subdomains was consistently high. Compared with the limited existing literature, these results contribute original evidence regarding the scale’s applicability within a different linguistic and cultural context and offer a more comprehensive perspective on its measurement properties.
Conclusion
This study evaluated the Turkish adaptation, validity, and reliability of the Gosnell Pressure Ulcer Risk Assessment Scale, originally developed by Davina J. Gosnell. Statistical analyses confirmed that the scale is both reliable and valid, supporting its use by healthcare professionals in Türkiye for assessing pressure ulcer risk.
Future research may explore the application of this scale in diverse healthcare settings and populations. Longitudinal studies are also needed to deepen our understanding of risk factors and preventive strategies for pressure ulcers. Such efforts would contribute to the development of more effective prevention and management approaches. Additionally, comparative clinical studies evaluating this scale against other pressure ulcer risk assessment tools could offer further insights and enrich the literature in this field.
One limitation of this study is the advanced age of the participants, which stems from the fact that the study was conducted in a palliative care unit. This factor may, albeit to a limited extent, influence the generalizability of the findings to other age groups and healthcare settings.
Furthermore, both exploratory and confirmatory factor analyses confirmed the unidimensional construct validity of the Turkish version of the Gosnell Pressure Ulcer Risk Assessment Scale. These results offer a solid empirical foundation supporting the use of the scale in Turkish clinical settings.
This study represents a notable contribution to the early detection and prevention of pressure ulcers, providing Turkish healthcare professionals with a validated and reliable tool. The findings underscore the importance of a multidisciplinary approach in pressure ulcer management and highlight the value of standardized assessment tools in enhancing healthcare outcomes.
Ethical approval
Ethical approval was obtained from the Non-Interventional Clinical Research Ethics Committee of Kütahya University of Health Sciences Faculty of Medicine (date: 14.09.2022, number: 2022/09-13). Written informed consent was obtained from the participants or their legal representatives.
Conflict of interest
The authors declare that there is no conflict of interest to disclose.
References
- Anders J, Heinemann A, Leffmann C, Leutenegger M, Pröfener F, von Renteln-Kruse W. Decubitus ulcers: pathophysiology and primary prevention. Dtsch Arztebl Int. 2010;107(21):371-381; quiz 382. https://doi.org/10.3238/arztebl.2010.0371
- Jalali R, Rezaie M. Predicting pressure ulcer risk: comparing the predictive validity of 4 scales. Adv Skin Wound Care. 2005;18(2):92-97. https://doi.org/10.1097/00129334-200503000-00013
- Reid J, Morison M. Classification of pressure sore severity. Nurs Times. 1994;90(20):46-50.
- Hajhosseini B, Longaker MT, Gurtner GC. Pressure injury. Ann Surg. 2020;271(4):671-679. https://doi.org/10.1097/SLA.0000000000003567
- Jaul E, Barron J, Rosenzweig JP, Menczel J. An overview of co-morbidities and the development of pressure ulcers among older adults. BMC Geriatr. 2018;18(1):305. https://doi.org/10.1186/s12877-018-0997-7
- Jaul E. Assessment and management of pressure ulcers in the elderly: current strategies. Drugs Aging. 2010;27(4):311-325. https://doi.org/10.2165/11318340-000000000-00000
- Kottner J, Cuddigan J, Carville K, et al. Prevention and treatment of pressure ulcers/injuries: The protocol for the second update of the international Clinical Practice Guideline 2019. J Tissue Viability. 2019;28(2):51-58. https://doi.org/10.1016/j.jtv.2019.01.001
- Bates-Jensen BM, Cheng J. Quality of care. Pressure ulcers in the aging population: a guide for clinicians. In: Thomas DR, Compton GA, editors. Totowa: Humana Press; 2014: 177-212.
- Gencer ZE, Ünal E, Özkan Ö. Basınç ülserleri tedavi maliyetleri etkililik analizi: konvansiyonel ve modern yara bakım tedavi maliyetlerinin karşılaştırılması. Akd Tıp D. 2019;5(2):201-208.
- Pancorbo-Hidalgo PL, Garcia-Fernandez FP, Lopez-Medina IM, Alvarez-Nieto C. Risk assessment scales for pressure ulcer prevention: a systematic review. J Adv Nurs. 2006;54(1):94-110. https://doi.org/10.1111/j.1365-2648.2006.03794.x
- Norton D, Exton-Smith AN, McLaren R. An investigation of geriatric nursing problems in hospital. London: Churchill Livingstone; 1962.
- Bergstrom N, Braden BJ, Laguzza A, Holman V. The braden scale for predicting pressure sore risk. Nurs Res. 1987;36(4):205-210.
- Waterlow J. Pressure sores: a risk assessment card. Nurs Times. 1985;81(48):49-55.
- Oğuz S, Olgun N. Braden Ölçeği ile hastaların risklerinin belirlenmesi ve planlı hemşirelik bakımının bası yaralarının önlenmesindeki etkinliğinin saptanması. Hemşirelik Forumu Derg. 1998;3(1):131-135.
- Pınar R, Oğuz S. Norton ve Braden bası yarası değerlendirme ölçeklerinin yatağa bağımlı aynı hasta grubunda güvenirlik ve geçerliliklerinin sınanması. VI. Ulusal Hemşirelik Kongresi; 1998.
- Avşar P, Karadağ A. Waterlow Basınç Ülseri Risk Değerlendirme Ölçeği’nin Türkçeye uyarlanması, geçerlik-güvenirlik çalışması. HUHEMFAD. 2016;3(3):1-15.
- Gosnell DJ. Pressure sore risk assessment: a critique. Part I. The Gosnell scale. Decubitus. 1989;2(3):32-38.
- Gosnell DJ. Pressure sore risk assessment. Part II. Analysis of risk factors. Decubitus. 1989;2(3):40-43.
- Gosnell DJ. Gosnell pressure sore risk assessment instrument revision. J Enterostomal Ther. 1989;16(6):272. https://doi.org/10.1097/00152192-198911000-00051
- Alpar R. Spor sağlık ve eğitim bilimlerinden örneklerle uygulamalı istatistik ve geçerlik-güvenirlik: SPSS’de çözümleme adımları ile birlikte. Ankara: Detay Yayıncılık; 2022: 527-638.
- Akman Ö, Ecevit Alpar Ş. Suriadi ve Sanada basınç yarası risk değerlendirme ölçeğinin Türkçe geçerlik ve güvenirliği. Hemşirelikte Araştırma Geliştirme Dergisi. 2014;16(1):1-11.
- Hancer M. Ölçeklerin yazım dilinden başka bir dile çevirileri ve kullanılan değişik yaklaşımlar. Balıkesir Üniversitesi Sosyal Bilimler Enstitüsü Dergisi. 2003;6(10):47-59.
- Yeşilyurt S, Çapraz C. Ölçek geliştirme çalışmalarında kullanılan kapsam geçerliği için bir yol haritası. Erzincan Üniversitesi Eğitim Fakültesi Dergisi. 2018;20(1):251-264. https://doi.org/10.17556/erziefd.297741
- Celdrán-Mañas M, Rueda-Lara MA, Gálvez-Toro A, Martínez-García R, Abizanda-Soler P. Validación de dos escalas de valoración del riesgo de úlceras por presión: Gosnell y Nova-4. Enfermería Viva. 1999;5(15):13-21.
Copyright and license
Copyright © 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.