Öz
Objective: The aim of this study was to investigate patients’ use of cytisine prescribed as a smoking cessation medication, the frequency of observed side effects, and smoking cessation rates at the Marmara University Family Medicine Smoking Cessation Clinic, thereby laying the groundwork for future research on cytisine use in Turkey.
Methods: The descriptive study included 256 participants who applied to the Marmara University Department of Family Medicine’s Smoking Cessation Clinic between May 2024 and March 2025 and underwent cytisine treatment. Participants’ sociodemographic characteristics, smoking status, cytisine use, and treatment processes were retrospectively collected via a questionnaire administered through telephone interviews. Tobacco dependence level was assessed using the Fagerström nicotine dependence test (FNDT). The dependent variable of the study is smoking cessation status; the independent variables are age, gender, education level, smoking burden, medication completion, and attendance at follow-up appointments. Data were analyzed using SPSS 25.0 software, and p<0.05 was considered statistically significant.
Results: The average age of participants was 40.7±0.9 years, the average FNDT score was 6.3±2.2, and the average smoking burden (pack/year) was 24.9±1.3. In our study, 31% of individuals who initiated cytisine treatment were not smoking at follow-up. The proportion of participants who remained non-smoking status at assessment was significantly higher among those with lower smoking burden, those who attended follow-up appointments, those with higher perceived income, and those who completed the medication (p=0.027, p=0.035, p≤0.001, p=0.020). In multivariable analysis, higher perceived income independently predicted non-smoking status at follow-up (aOR=1.91, p=0.004), whereas treatment completion showed borderline significance.
At least one side effect was observed in 31.5% (n=79) of participants; the most commonly reported were nausea (10.2%), palpitations (3.9%), dizziness (3.5%), and mood changes (3.5%).
Conclusion: In this real-world clinical setting, 31% of patients receiving cytisine were classified as non-smokers at follow-up. In the context of limited national data, these results offer exploratory evidence to guide the design of future randomized controlled trials.
Anahtar Kelimeler: cytisine, nicotine addiction, smoking cessation
Introduction
Tobacco use is a major public health threat worldwide, causing more than 8 million deaths each year. More than 7 million of these deaths are directly related to diseases caused by tobacco consumption, such as lung cancer, ischemic heart disease, stroke, and chronic obstructive pulmonary disease. Approximately 1.3 million people die each year from exposure to secondhand smoke without ever having smoked themselves.[1,2] Today, nicotine replacement therapy (NRT), varenicline, and bupropion are considered the most effective methods for quitting smoking.[3] A lesser-known drug is cytisine, a plant-based alkaloid derived from the seeds of Cytisus laburnum (golden rain acacia), which was approved as a smoking cessation treatment in Bulgaria in 1964.[4] Although the popularity of cytisine has fluctuated over time, its use has increased markedly in recent years.[3] Recent clinical studies have demonstrated cytisine's effectiveness in smoking cessation, and this drug has been included in the World Health Organization's Clinical Practice Guideline on Smoking Cessation in Adults.[5] Cytisine has a strong affinity for the α4β2 subtype receptor and acts as a partial agonist of the acetylcholine nicotinic cholinergic receptor.[6] Studies have shown that cytisine has a relatively short elimination half-life of about 4.8 hours, and nearly all of the compound (around 95%) is eliminated unchanged through the urine. A notable feature of its pharmacokinetic profile is that it undergoes virtually no hepatic metabolism.[7] It may help alleviate nicotine withdrawal symptoms. These characteristics make cytisine a cost-effective treatment for smoking cessation.[8]
The recommended dosage regimen for cytisine used in our country is a 25-day tapering regimen, starting with six tablets daily at 2-hour intervals, followed by gradual dose reduction throughout treatment.[9]
The most commonly reported side effects are nausea, vomiting, insomnia, taste changes, dry mouth and throat, loss of appetite, and a slight increase in blood pressure. It has also been noted that high doses of cytisine may cause dizziness and muscle weakness.[3,5] However, it has been shown that reducing the dose alleviates these side effects, and symptoms resolve after discontinuation of the drug. Cytisine does not cause psychophysical changes and is therefore considered a safe option for people who drive or operate machinery.[8]
In a randomized controlled trial comparing cytisine with placebo, cytisine was found to have higher smoking cessation rates compared to placebo. In follow-ups lasting longer than 6 months, cytisine was found to promote longer smoking cessation and showed no significant difference from placebo in terms of serious side effects.[6]
In a study conducted in Australia, cytisine treatment administered for 25 days was compared with 84-day varenicline treatment in smokers motivated to quit. Cytisine was reported to show smoking cessation outcomes comparable to varenicline and was associated with fewer reported adverse effects and lower treatment discontinuation rates.[10,11] Some systematic reviews and indirect comparisons have also suggested that cytisine may have a more favorable adverse effect profile compared with bupropion; however, these findings should be interpreted cautiously because of the indirect nature of the comparisons, heterogeneity between studies, and varying levels of evidence certainty.[12,13]
In another study conducted among individuals motivated to quit smoking, cytisine was associated with higher smoking cessation rates than NRT. Participants in the cytisine group reported fewer withdrawal symptoms, reduced cigarette consumption, and a longer time to relapse. However, self-reported adverse effects during the 6-month follow-up period were approximately twice as common in the cytisine group compared with the NRT group.[14,15]
Based on research and clinical practice results, cytisine can be considered a promising option for smoking cessation treatment, as it is less expensive than other treatment options and effective in alleviating nicotine withdrawal symptoms.[16] A systematic review also indicated that new studies are needed to explore the balance between the advantages of accessibility and affordability in low- and middle-income economies and the modest efficacy demonstrated for cytisine to date.[17]
It is available as a generic or prescription drug in at least 18 countries. In Canada, it was licensed as an over-the-counter natural health product in 2017 and began to be sold by prescription in the UK in January 2024.[7,18] In Turkey, since 2024, it has been provided by the Ministry of Health and distributed to patients with appropriate indications free of charge and without a prescription through the Tobacco Addiction Treatment Monitoring System (TUBATİS).[19] Since then, cytisine has been used in patients who have applied to quit smoking to the Department of Family Medicine’s Smoking Cessation Clinic of Marmara Pendik Education and Research Hospital.
There is limited national data regarding cytisine, which has only recently been introduced for smoking cessation treatment in our country. The aim of this study was to investigate patients’ use of cytisine prescribed as a smoking cessation medication, the frequency of observed side effects, and smoking cessation rates. Furthermore, due to the limited availability of national data on cytisine use, this study is expected to contribute to the literature.
Materials and Methods
This research is a descriptive study conducted between April 2025 and July 2025.
Setting and sample size
The study population consists of all patients who applied to the Marmara University Department of Family Medicine’s Smoking Cessation Clinic between May 2024 and March 2025 and received cytisine treatment. It was aimed to reach the entire population without sampling.
Inclusion and exclusion criteria
Participants aged 18–65 years who initiated cytisine treatment were included in the study, as cytisine is approved for use within this age range. Patients who obtained the medication but did not use it were excluded from the study. In addition, patients receiving additional pharmacological treatments that could affect smoking cessation outcomes, including antidepressants and other smoking cessation medications, were not included in the study. No participants reported electronic cigarette use at the time of admission.
Design of study
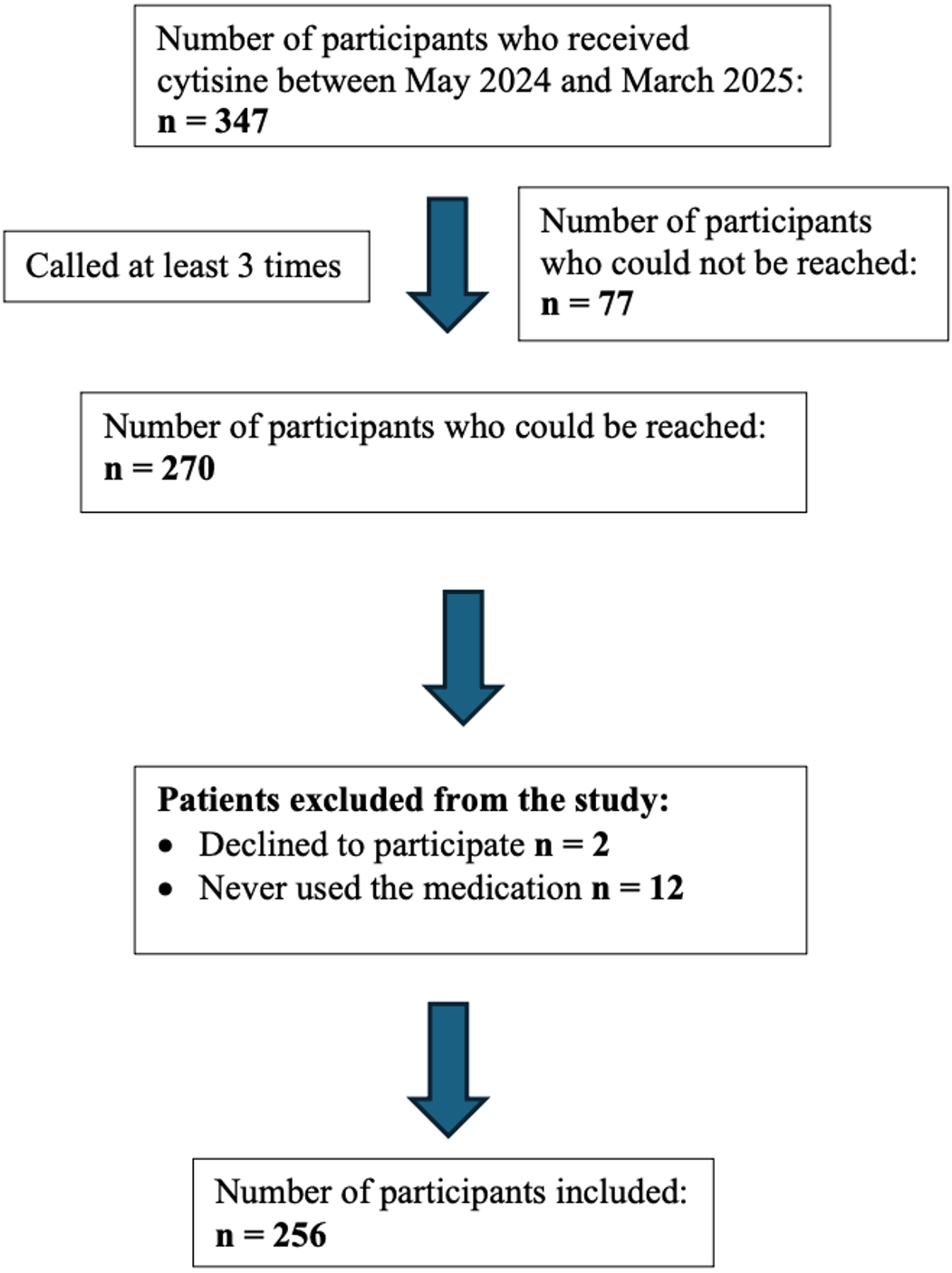
Researchers contacted 347 patients who applied to the Marmara University Department of Family Medicine’s Smoking Cessation Clinic between May 2024 and March 2025 and underwent cytisine treatment via the contact numbers registered in the system. During the study period, 642 patients attended the smoking cessation clinic; 347 received cytisine, 22 bupropion, 218 nicotine replacement therapy (NRT), and 55 did not receive any medication/NRT.
Participants were read the voluntary information and consent form, and those who verbally agreed to participate in the study were included in the research. Those who did not answer the call were called at least three times on consecutive days. Seventy-seven participants did not answer the calls, and two did not wish to participate in the study. Twelve participants were excluded from the study because they had never used cytisine treatment. The study was completed with 256 participants. A schematic representation of the sample obtained at the end of the study is shown in Figure 1.
Researchers administered a 15-question survey to participants during a telephone interview, which included questions about their sociodemographic characteristics, smoking cessation status, development of side effects, medication completion status, and attendance at follow-up appointments. Smoking status was assessed based on participants’ self-reports. At follow-up, participants were asked directly whether they were still smoking or had quit smoking, and smoking cessation status was classified accordingly. No biochemical verification was performed. The questions were read aloud by the researcher during the interview. The patient's level of dependence was assessed using the Fagerström nicotine dependence test (FNDT) score available in the system. The Turkish validity and reliability of the FNDT have previously been demonstrated.[20] The scores were classified as ‘0-4 points’ for low dependence, ‘5 points’ for moderate dependence, and ‘6-10 points’ for very high dependence.[1,16]
The dependent variable of the study is the patients' current smoking status. The independent variables are the patients' age, gender, education level, smoking burden (pack/year), medication completion status, and status of attendance at follow-up visit.
Data analysis
SPSS for Windows 25.0 software was used for statistical analysis and data recording. Data showing a normal distribution are presented as mean ± standard deviation (SD), while data not showing a normal distribution are presented as median (minimum–maximum) values. Categorical data are presented as number (n) and percentage (%). Perceived income was initially recorded in three categories; however, for regression analysis, it was recategorized into two groups due to the limited number of participants in some categories and to improve model stability. Normal distribution was assessed using visual (graphs) and analytical methods (Kolmogorov–Smirnov/Shapiro–Wilk tests). The Mann–Whitney U test was used to compare two independent groups in non-normally distributed data, while the independent samples t-test was used for normally distributed data. The chi-square test was applied to compare categorical data. To identify factors associated with smoking cessation, multivariable logistic regression analysis was performed. Missing data for perceived income and FNDT score were handled using multiple imputation with fully conditional specification. Five imputed datasets were generated, and pooled regression estimates were calculated according to Rubin’s rules. Adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were reported. p<0.05 was accepted as the level of statistical significance. The manuscript was prepared in accordance with the relevant STROBE recommendations for observational studies.
Research ethics committee application and required permissions
Approval for the study was obtained from Marmara University Faculty of Medicine Clinical Research Ethics Committee (Protocol code: 09.2025.25-0320)
Results
In the study, 36.3% (n=93) of participants were female, and 63.7% (n=163) were male. The average age of participants was 40.7 ± 0.9. According to the FNDT, 19.8% (n=47) of participants are low level, 13.9% (n=33) are medium level, and 66.2% (n=157) are high level dependent. The mean FNDT score is 6.3 ± 2.2. The mean smoking burden (pack/year) of participants is 24.9 ± 1.3. Following medication use, 31% (n=79) of participants had quit smoking, while 69% (n=177) continued to smoke. The characteristics of all participants in the study, including smoking cessation status and characteristics related to cytisine use, are shown in Table 1.
|
Numbers of the participants did not provide a response = a:7 b:10 c:11 d:51 e:21 f:17 g:22 h:6 ı:5 j:5 *Valid percentage is used** Employment status was recategorized as employed/not employed for analysis due to small cell counts; the not employed group included unemployed participants, students, retirees, and homemakers. |
|||
| Table 1. Sociodemographic characteristics, smoking cessation status, and treatment-related characteristics of the participants | |||
| Variable | Category |
|
|
| Marital Status a | Single/Divorced/Widowed |
|
|
| Married |
|
|
|
| Education b | Middle school or below |
|
|
| High school or above |
|
|
|
| Employment Status c** | Unemployed |
|
|
| Employed |
|
|
|
| Perceived Income d | Income < Expenses |
|
|
| Income = Expenses |
|
|
|
| Income > Expenses |
|
|
|
| Living Arrangement e | Alone |
|
|
| With spouse / children / others |
|
|
|
| Alcohol Consumption f | Yes |
|
|
| No |
|
|
|
| Physical Activity g | Yes |
|
|
| No |
|
|
|
| Chronic Disease h | Absent |
|
|
| Present |
|
|
|
| Smoking cessation status | Non-smoking |
|
|
| Smoking |
|
|
|
| Side effect i | Yes |
|
|
| No |
|
|
|
| Cytisine completion status j | Yes |
|
|
| No |
|
|
|
Participants with a lower average smoking burden (pack-years) and those who attended follow-up examinations were more likely to report not currently smoking at the time of contact compared to others (p=0.027 and p=0.035, respectively). Furthermore, individuals with a high perceived income were more likely to report not currently smoking than those with a balanced or low perceived income (p<0.001). Factors that may affect participants' smoking status when using cytisine are presented in Table 2.
|
*Valid percentage is used **FNDT: Fagerström Nicotine Dependence Numbers of the participants did not provide a response a:10, b: 51, c:17, d:7. Independent Samples t-test and Pearson Chi-Square Test was used. Perceived income was recategorized for analysis. |
|||
| Table 2. Categorical and continuous factors associated with non-smoking status | |||
| Factor |
n (%)* |
n (%)* |
|
| Attending follow-up visits |
|
||
| Yes |
|
|
|
| No |
|
|
|
| Completion of treatment |
|
||
| Yes |
|
|
|
| No |
|
|
|
| Difficulty following medication doses |
|
||
| Disagree |
|
|
|
| Agree |
|
|
|
| Previous quit attempts |
|
||
| Yes |
|
|
|
| No |
|
|
|
| Side effects |
|
||
| Yes |
|
|
|
| No |
|
|
|
| Education level a |
|
||
| Middle school or below |
|
|
|
| High school or above |
|
|
|
| Perceived income status b |
|
||
| Income ≤ expenses |
|
|
|
| Income > expenses |
|
|
|
| Alcohol use c |
|
||
| Yes |
|
|
|
| No |
|
|
|
| Chronic disease history d |
|
||
| Yes |
|
|
|
| No |
|
|
|
|
|
|
||
| Age |
|
|
|
| FNDT** score |
|
|
|
| Smoking load (pack-years) |
|
|
|
The multivariable logistic regression model was statistically significant (Omnibus test χ2(5)=15.03, p=0.010). Model fit was acceptable according to the Hosmer–Lemeshow test (χ2=14.24, p=0.076). The model explained approximately 11% of the variance in non-smoking status (Nagelkerke R2=0.112). In the multivariable logistic regression model, higher perceived income (aOR=1.91, 95% CI 1.23–2.96, p=0.004) remained independently associated with non-smoking status at follow-up, whereas treatment completion (aOR=1.93, 95% CI 0.98-3.83, p=0.059) showed a borderline association and other variables were not independently associated (Table 3).
|
Model statistics: Omnibus test of model coefficients: p < 0.05, Hosmer–Lemeshow test: p > 0.05 across imputations, Nagelkerke R2 ≈ 0.11 Multiple imputation: Fully conditional specification, 5 imputations; missingness: perceived income 19.9%, FNDT 7.8%; pooled according to Rubin’s rules.B: Regression Coefficient SE: Standard Error OR: Odds Ratio Perceived income was recategorized for regression analysis. |
||||
| Table 3. Multivariable logistic regression analysis of factors associated with non-smoking status (multiple imputation, pooled results, n=256) | ||||
| Variable |
|
|
|
|
| Treatment completion |
|
|
|
|
| Perceived income |
|
|
|
|
| FNDT score |
|
|
|
|
| Smoking load(pack-years) |
|
|
|
|
| Follow-up attendance |
|
|
|
|
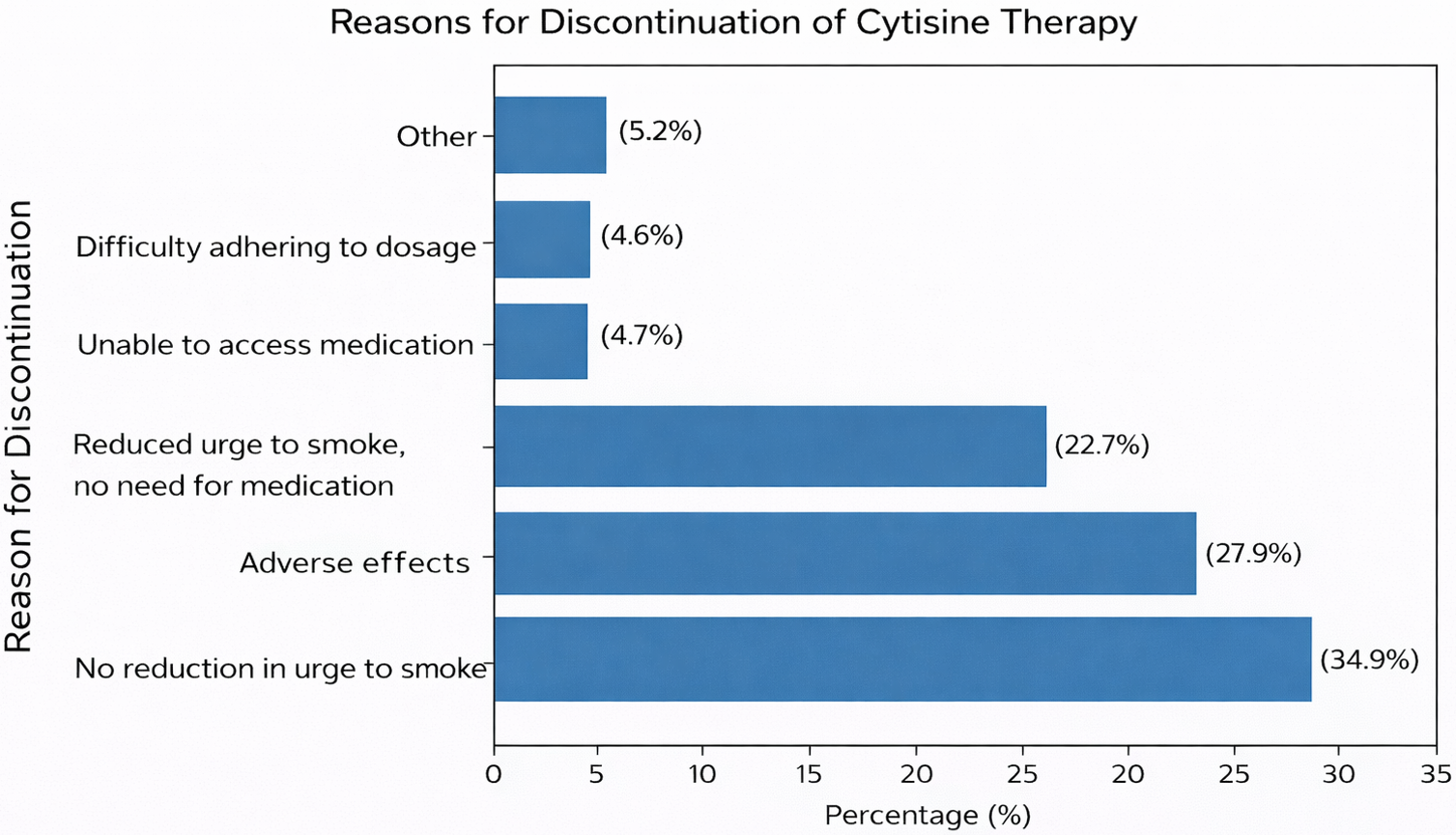
Among the participants, 44.2% completed the medication, while 55.8% did not. A higher proportion of those who completed the medication reported not currently smoking compared to those who did not complete the treatment (p=0.020). Among participants who did not complete the treatment, the median duration of medication use was 7 days (range: 1–24 days). Participants who stated that they “did not have difficulty following the medication doses”, attended more follow-ups, and experienced fewer side effects were statistically significantly more likely to complete the medication (p=0.028, p<0.001, p<0.001, respectively). The median duration of use among non-completers was 7 days (min: 1 day, max: 24 days). The reasons for discontinuing the medication among participants who did not complete the treatment were as follows; 34.9% stated “No reduction in the urge to smoke”, 27.9% stated ‘Side effects’, 22.7% stated “A reduction in the urge to smoke, did not need the medication”, 4.7% stated “The medication was left at another home/city/location and I could not access it”, and 4.6% stated “I had difficulty following the medication dosage.” Factors that could affect participants' completion of the drug are listed in Table 4.
|
Pearson Chi-Square Test was used Numbers of the participants did not provide a response= a: 27, b:13, c:7, d:11, e:21 *Valid percentage is used |
|||
| Table 4. Factors Associated with Completion of Cytisine Treatment | |||
| Factor |
n (%)* |
n (%)* |
|
| “I had difficulty following the medication doses” a |
|
||
| Disagree |
|
|
|
| Agree |
|
|
|
| Attending follow-up visits b |
|
||
| Did not attend |
|
|
|
| Attended |
|
|
|
| Side effects during cytisine use c |
|
||
| Yes |
|
|
|
| No |
|
|
|
| Chronic disease history d |
|
||
| Yes |
|
|
|
| No |
|
|
|
| Alcohol use e |
|
||
| Yes |
|
|
|
| No |
|
|
|
Following medication use, 31.5% of participants (n=79) experienced at least one side effect, at least once. The most commonly observed side effects were nausea 10.2% (n=26), palpitations 3.9% (n=10), dizziness 3.5% (n=9), and mood changes 3.5% (n=9).While nausea was the most frequent adverse effect, chest pain resulted in the highest rate of drug discontinuation when it occurred (n =4, 80%).The incidence of side effects and discontinuation of medication due to side effects among participants is shown in Table 5. Among participants who did not complete the treatment, the most common reason for medication discontinuation was “lack of reduction in the urge to smoke” (34.9%). This was followed by “adverse effects” (27.9%) and “unwillingness to continue the medication once a reduction in the urge to smoke was achieved” (22.7%) (Figure 2).
| Some participants experienced more than one side effect. | |||
| Table 5. Side effect and treatment discontinuation due to side effect among participant | |||
| Side effect |
|
|
|
|
|
|
||
| Nausea |
|
|
|
| Palpitations |
|
|
|
| Dizziness |
|
|
|
| Mood changes |
|
|
|
| Heartburn / epigastric pain |
|
|
|
| Sleep disturbances |
|
|
|
| Dry mouth |
|
|
|
| Chest pain |
|
|
|
| Fatigue |
|
|
|
| Other(diarrhea,itching eg.) |
|
|
|
Discussion
In our study, 31% of individuals who initiated cytisine treatment reported abstinence from smoking. Among the participants, 44.2% completed the full drug dosage regimen. The most frequently reported side effect was nausea; however, chest pain was the symptom most commonly leading to treatment discontinuation. The present study demonstrated a significant association between smoking abstinence and higher perceived income level, treatment completion, attendance at follow-up visits, and smoking burden. In the multivariable logistic regression model, higher perceived income (aOR=1.91, p=0.004) remained independently associated with non-smoking status at follow-up, whereas treatment completion (aOR=1.93, p=0.059) showed borderline statistical significance, and the other variables were not independently associated with the outcome. This association may reflect differences in psychosocial resources, treatment adherence, health literacy, or access to supportive environments.
In the literature, smoking cessation rates associated with cytisine are generally similar to those observed in our study, although lower rates have also been reported. Walker et al. reported 6-month smoking cessation rates of 22% for cytisine and 15% for NRT.[4] In another study by the same authors, comparing cytisine with varenicline, cessation rates were 22.9% and 17.5%, respectively.[15] A review reported successful smoking cessation in approximately 18–23% of individuals using cytisine.[17] In a study evaluating biochemically verified abstinence at 6 months, smoking cessation rates were reported as 50.5% for cytisine, 55.9% for varenicline, and 51.0% for NRT.[11] The higher cessation rates observed in that study may be related to differences in treatment duration, behavioral support, and study design.
A retrospective study from Türkiye reported that 61.5% of patients receiving cytisine achieved smoking cessation during the early treatment period.[21] Differences in study design, follow-up duration, and outcome assessment methods may explain the higher cessation rates compared with our findings. Since our study had a descriptive and cross-sectional design, smoking cessation status and follow-up periods varied among participants. Therefore, comparisons with long-term outcomes from randomized controlled trials should be interpreted cautiously.
In our study, 31.5% of participants experienced at least one side effect during cytisine treatment. Walker et al. reported that comparing varenicline with cytisine, the proportion of participants experiencing the most common adverse effects was 32%, which is similar to our study.[4] The most common side effect in our study was nausea, occurring in 10.2% (n=26) of participants. Gastrointestinal adverse effects, particularly nausea, were among the most commonly reported side effects associated with cytisine treatment in previous studies and systematic reviews.[17] In the study by Vinnikov et al.; dyspepsia, nausea, and headache were the most common side effects in the cytisine group.[22] In the study by West et al. comparing cytisine with placebo, gastrointestinal complaints were more common in the cytisine group than in the placebo group.[6] In the study by Walker et al., side effects such as nausea, vomiting, and sleep disturbances were significantly more common in the cytisine group compared to the NRT group (4.6% vs. 0.03%; p=0.0002).[15] In the study by Rigotti et al., adverse events were reported in 4.4% of patients in the cytisine group, with gastric complaints, headache, and sleep disturbances being the most common. (1.4%, 0.9%, and 0.5%, respectively).[23]
In our study, palpitations were observed in 3.9% (n = 10) of participants, making it the second most common side effect. In one study included in a meta-analysis, tachycardia was reported in 62 of 388 patients (16%), while in another, mild tachycardia was reported in 3 of 70 patients (4%).[24] In our study, 50% of participants who experienced palpitations discontinued the drug because of this side effect; no similar information was found in the literature. Drug-related side effects may reduce treatment adherence and may be associated with lower smoking cessation rates. Therefore, careful monitoring and patient counselling regarding potential adverse effects may be important during treatment. Differences in adverse event rates across studies may also reflect variations in study populations, adverse event reporting methods, and treatment protocols.
Limitations and strengths: Due to the single-center, descriptive, and cross-sectional design of the study, causal relationships could not be established and no control group was included. This limits the comparative interpretation and generalizability of the findings, as well as the ability to clearly demonstrate the effect of the intervention. Additionally, the retrospective nature of data collection may have introduced recall bias and resulted in incomplete responses to some questions. The absence of biochemical verification and reliance solely on self-reported smoking status represent additional limitations. Furthermore, only short-term smoking status at follow-up was assessed; therefore, no conclusions can be drawn regarding the long-term effectiveness of cytisine in maintaining smoking abstinence. Because the interval between treatment initiation and telephone assessment varied among participants, follow-up duration was not uniform across the study population.
While most studies in the literature focus on patients who completed the full treatment protocol—typically defined as using the medication for at least 25 days—our study included individuals who attended the smoking cessation clinic and used cytisine for at least one day (1 tablet every 2 hours, 6 tablets per day). Although this approach does not allow conclusions regarding the full treatment regimen, it provides real-world information about patients who discontinued treatment early.
Of the 347 patients who initiated cytisine treatment, 256 were included in the final analysis. Missing data from the remaining participants may have influenced the observed smoking cessation rates. If all non-respondents had continued smoking, the proportion of non-smoking participants would decrease from 31% to 22.8%. Therefore, the true proportion of non-smoking likely lies between 22.8% and 31%, depending on the smoking status of non-respondents. Because baseline demographic and dependence characteristics of non-respondents were unavailable, formal comparisons could not be performed. If non-respondents had higher nicotine dependence, lower adherence, or lower motivation, the observed smoking cessation proportion may represent an overestimate. Therefore, the findings should be interpreted cautiously in light of potential selection bias.
Only variables measured in this study were included in the regression model. However, unmeasured factors such as motivation to quit smoking, psychiatric comorbidities, and counseling or social support may also have influenced treatment adherence and smoking cessation outcomes. Therefore, the results should be interpreted with possible residual confounding in mind.
Conclusion
This study provides real-world data regarding the short-term smoking status and tolerability of cytisine treatment in a family medicine smoking cessation clinic. Approximately one-third of participants reported non-smoking status at follow-up. These findings suggest that cytisine may represent a feasible and accessible smoking cessation option in primary care settings.
Further studies with larger sample sizes, randomized controlled designs, and longer follow-up periods are needed to better evaluate the long-term effectiveness of cytisine in smoking cessation clinics in our country. In addition, future studies evaluating cytisine together with counseling support in primary care settings may provide further insight into treatment adherence and sustained smoking cessation outcomes.
Ethical approval
Approval for the study was obtained from Marmara University Faculty of Medicine Clinical Research Ethics Committee with the protocol code 09.2025.25-0320 dated 18.04.2025.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest to disclose.
Acknowledgments
We would like to express our sincere gratitude to all participants of the Family Medicine Smoking Cessation Clinic for their valuable contributions to this study.
Declaration of generative AI and AI-assisted technologies in the writing process
During the revision of this manuscript in May 2026, the artificial intelligence program ChatGPT was used only to assist with language editing, grammar correction, and improving clarity of expression. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Referanslar
- World Health Organization (WHO). Global report on trends in prevalence of tobacco use 2000–2030. 2024. Available at: https://iris.who.int/server/api/core/bitstreams/1903bfca-6c2f-470c-bd52-237edf4828ca/content (Accessed on 14 October 2025).
- Jha P, Ramasundarahettige C, Landsman V, et al. 21st-Century Hazards of Smoking and Benefits of Cessation in the United States. NEJM. 2013;368(4):341-50. https://doi.org/10.1056/NEJMsa1211128
- Nur Savran F, Küçükceran H, Gökşin Cihan F, Demirbaş N, Karaoğlu N. Cytisine treatment in nicotine addiction. The Journal of Turkish Family Physician. 2025;16(2):124-136. https://doi.org/10.15511/tjtfp.25.00224
- Walker N, Smith B, Barnes J, et al. Cytisine versus varenicline for smoking cessation in New Zealand indigenous Māori: a randomized controlled trial. Addiction. 2021;116(10):2847-2858. https://doi.org/10.1111/add.15489
- World Health Organization (WHO). Clinical treatment guideline for tobacco cessation in adults. 2024. Available at: https://iris.who.int/server/api/core/bitstreams/2deb01bc-1be9-4e9c-b113-5efbb67780c7/content (Accessed on 14 October 2025).
- West R, Zatonski W, Cedzynska M, et al. Placebo-controlled trial of cytisine for smoking cessation. N Engl J Med. 2011;365:1193-1200. https://doi.org/10.1056/NEJMoa1102035
- Reddy KP, Paltiel AD, Freedberg KA, Rigotti NA. Public health impact of FDA’s request for additional safety data on cytisine for tobacco cessation. JAMA Health Forum. 2024;5(8):e242647. https://doi.org/10.1001/jamahealthforum.2024.2647
- Torazzi A, Tedesco E, Ceccato S, et al. Safety and efficacy of CyTisine for smoking cessation in a hOSPital context (CITOSP): study protocol for a prospective observational study. Front Public Health. 2024;12:1350176. https://doi.org/10.3389/fpubh.2024.1350176
- Kızıltaş Ö. Türkiye'de sigara bırakmada yeni medikal tedavi: sitizin. Bağımlılık Dergisi. 2025;26(2):274-276. https://doi.org/10.51982/bagimli.1603413
- Courtney RJ, McRobbie H, Tutka P, et al. Effect of cytisine vs varenicline on smoking cessation: a randomized clinical trial. JAMA. 2021;326(1):1-10. https://doi.org/10.1001/jama.2021.7621
- Tinghino B, Cardellicchio S, Corso F, et al. Cytisine for smoking cessation: a 40-day treatment with an induction period. Tob Prev Cessat. 2024;10:23. https://doi.org/10.18332/tpc/187556
- Shang X, Guo K, E. F, et al. Pharmacological interventions on smoking cessation: a systematic review and network meta-analysis. Front Pharmacol. 2022;13:1012433. https://doi:10.3389/fphar.2022.1012433
- Livingstone-Banks J, Lindson N, Hartmann-Boyce J. Effects of interventions to combat tobacco addiction: Cochrane update of 2021 to 2023 reviews. Addiction. 2024;119(12):2101-2115. https://doi.org/10.1111/add.16624
- Ofori S, Lu C, Olasupo OO, et al. Cytisine for smoking cessation: a systematic review and meta-analysis. Drug Alcohol Depend. 2023;251:110936. https://doi.org/10.1016/j.drugalcdep.2023.110936
- Walker N, Howe C, Glover M, et al. Cytisine versus nicotine for smoking cessation. NEJM. 2014;371(25):2353-2362. https://doi.org/10.1056/NEJMoa1407764
- Etter JF, Lukas RJ, Benowitz NL, et al. Cytisine for smoking cessation: a research agenda. Drug Alcohol Depend. 2008;92(1-3):3-8. https://doi.org/10.1016/j.drugalcdep.2007.06.017
- Livingstone-Banks J, Fanshawe TR, Thomas KH, et al. Nicotine receptor partial agonists for smoking cessation. Cochrane Database Syst Rev. 2023;5(5):CD006103. https://doi.org/10.1002/14651858.CD006103.pub8
- Karnieg T, Wang X. Cytisine for smoking cessation. CMAJ. 2018;190(19):E596. https://doi.org/10.1503/cmaj.171371
- T.C. Sağlık Bakanlığı, Halk Sağlığı Genel Müdürlüğü. Ülkemizdeki tütün kontrol çalışmaları. 2024. Available at: https://havanikoru.saglik.gov.tr/tuetuen-hakkinda/uelkemizdeki-tuetuen-kontrol-calismalari.html (Accessed on Feb 2, 2026).
- Uysal MA, Kadakal F, Karşidağ Ç, et al. Fagerstrom test for nicotine dependence: reliability in a Turkish sample and factor analysis. Tuberk Toraks. 2004;52(2):115-121. Available at: https://www.tuberktoraks.org/managete/fu_folder/2004-02/2004-52-2-115-121.pdf (Accessed on May 24, 2026).
- Gökseven Arda Y, Kocatürk Güllü E, Zeren Öztürk G. Effectiveness of pharmacological smoking cessation treatments: a retrospective comparison of common methods. Turk J Fam Pract. 2025;29(3):167-177. https://doi.org/10.54308/turkjfampract.2025.877
- Vinnikov D, Brimkulov N, Burjubaeva A. A Double-blind, randomized, placebo-controlled trial of cytisine for smoking cessation in medium-dependent workers. J Smok Cessat. 2008;3(1):57-62. https://doi.org/10.1375/jsc.3.1.57
- Rigotti NA, Benowitz NL, Prochaska J, et al. Cytisinicline for smoking cessation: a randomized clinical trial. JAMA. 2023;330(2):152. https://doi.org/10.1001/jama.2023.10042
- Etter JF. Cytisine for smoking cessation: a literature review and a meta-analysis. Arch Intern Med. 2006;166(15):1553-1559. https://doi.org/10.1001/archinte.166.15.1553
Telif hakkı ve lisans
Telif Hakkı © 2026 Yazar(lar). Açık erişimli bu makale, orijinal çalışmaya uygun şekilde atıfta bulunulması koşuluyla, herhangi bir ortamda veya formatta sınırsız kullanım, dağıtım ve çoğaltmaya izin veren Creative Commons Attribution License (CC BY) altında dağıtılmıştır.