Öz
Objective: Primary healthcare services constitute the initial point of contact within the healthcare system and play a fundamental role in terms of efficiency, evidence-based decision-making, and sustainability. Within the scope of the “Digital Transformation and Integration System in Healthcare,” developed to enhance the effectiveness of the family medicine system in Türkiye and ensure service integration, a contact registration desk and a Family Medicine Convenience Polyclinic have been established at our center. This study aims to evaluate the demographic and clinical characteristics, reasons for presentation, and patient satisfaction levels of individuals presenting to the registration desk located in the Family Medicine Convenience Polyclinic.
Methods: This cross-sectional study included 312 patients who presented to the registration desk at the Family Medicine Convenience Polyclinic of Gülhane Training and Research Hospital between January 1, 2025, and June 30, 2025. Data were obtained from the hospital information management system and a questionnaire form prepared in accordance with the literature. The Patient Satisfaction Assessment Short Form (PSASF) consists of seven items on a 5-point Likert scale, with higher scores indicating greater levels of dissatisfaction. Chi-square, Fisher’s exact, and Mann-Whitney U tests were used in the data analysis; significant variables were included in multivariate logistic regression analysis. Based on G*Power analysis (80% power, α=0.05), a minimum of 250 participants was deemed sufficient; 312 patients found suitable during the study period were included in the analyses.
Results: The median age of participants was 45 years, and 79.8% were female; 40.7% were university graduates, 44.2% had at least one chronic disease, and 76.6% of applications were for radiological examination purposes. The overall satisfaction rate is 92.6%, with the highest satisfaction related to the respectful attitude of the healthcare staff (66.0%) and the lowest satisfaction related to the time spent with the doctor (33.0%). When comparing satisfied and dissatisfied groups, female gender (p=0.019), advanced age (p<0.001), low education level (p=0.050), and the presence of chronic disease (p=0.024) were found to be significantly related to satisfaction, while no significant difference was found in terms of the reason for referral (p=0.064). In the univariate model of the logistic regression analysis, age (p=0.001), gender (p=0.023), education level (p=0.052), comorbidities (p=0.031), and reason for referral (p=0.070) were found to be associated with satisfaction; while in the multivariate analysis, only being in the ≥45 age group was shown to be independently associated with satisfaction (OR=9.77; 95% CI: 1.80–53.06; p=0.008).
Conclusion: The “Digital Transformation and Integration System in Healthcare” model has been demonstrated to increase efficiency in the healthcare system and strengthen patient satisfaction. The findings indicate that expanding digital integration may provide significant contributions to improving accessibility, service quality, and inclusivity in primary healthcare services.
Anahtar Kelimeler: family medicine, patient satisfaction, digital integration, primary healthcare services
Introduction
Primary healthcare services constitute the initial point of contact for individuals within the healthcare system and represent a fundamental component of an effective, accessible, and sustainable healthcare framework. The robust delivery of these services is critically important for preserving public health, supporting evidence-based decision-making processes, and ensuring the efficient utilization of healthcare resources. The World Health Organization (WHO) emphasizes that strong primary healthcare services are indispensable for the continuity and effectiveness of healthcare systems.[1,2] In Türkiye, the Family Medicine System (FMS), implemented in 2010, aims to provide integrated, continuous, and patient-centered primary healthcare services. The system ensures easy access for every citizen to preventive, curative, and rehabilitative health services through an assigned family physician.[3] In conjunction with the Health Transformation Program, the restructuring of primary healthcare services has enabled the holistic delivery of preventive and curative services. The widespread adoption of the Family Medicine model has contributed to increased patient satisfaction, improved access to services, and strengthened physician-patient communication.[4]
Various studies have reported that some individuals utilize family medicine services to a limited extent or prefer to apply directly to hospitals. The restricted availability of laboratory and imaging facilities within Family Health Centers (FHCs) leads to delays in diagnostic and treatment processes, necessitating referrals to secondary or tertiary healthcare institutions.[5] This situation is associated with a lack of awareness regarding service access, inadequacies in referral processes, and deficiencies in intra-system coordination.[5,6] Consequently, unnecessary referrals may result in both time loss and wastage of workforce and resources within the healthcare system.[7] To mitigate these issues and ensure comprehensive integration in healthcare services, the Ministry of Health of the Republic of Türkiye has implemented the “Digital Transformation and Integration System.” This system has facilitated digital data flow between primary healthcare institutions and secondary and tertiary hospitals; additionally, a new initiative named “Family Medicine Convenience Polyclinics” has been developed. These polyclinics are structures where family physicians can refer patients for advanced examinations and evaluations while also providing access to laboratory and imaging services.[8] Thus, direct applications by patients to secondary or tertiary institutions are prevented; the service capacity of family physicians is enhanced, and efficiency within the healthcare system is achieved. This model has the potential to increase efficiency in administrative and clinical decision-making processes by accelerating transitions between primary care and hospital services.
International literature demonstrates that enhancing the competencies of primary care physicians reduces unnecessary referrals, improves service quality, and contributes to the overall cost-effectiveness of the healthcare system.[9,10] In this context, evaluating the field applicability and impact on patient satisfaction of innovative models such as Family Medicine Convenience Polyclinics becomes increasingly important. The aim of this study is to analyze the sociodemographic characteristics, reasons for presentation, referral sources, and performed examinations of patients presenting to the registration desk of the Family Medicine Convenience Polyclinic established under the “Digital Transformation and Integration System,” and to elucidate the contributions of this new system to access to healthcare services and referral processes. The findings are expected to contribute to the development of primary healthcare services and to the more efficient utilization of resources within the system.
Materials and Methods
This study encompasses patients who presented to the registration desk of the Family Medicine Convenience Polyclinic at Gülhane Training and Research Hospital between January 1, 2025, and June 30, 2025. Using the hospital information management system, a list of patients who presented to the polyclinic during the specified period was generated, and individuals on the list were contacted by telephone to be informed about the study. Written informed consent was obtained from participants who agreed to participate; those unable to provide written consent were included upon verbal consent.
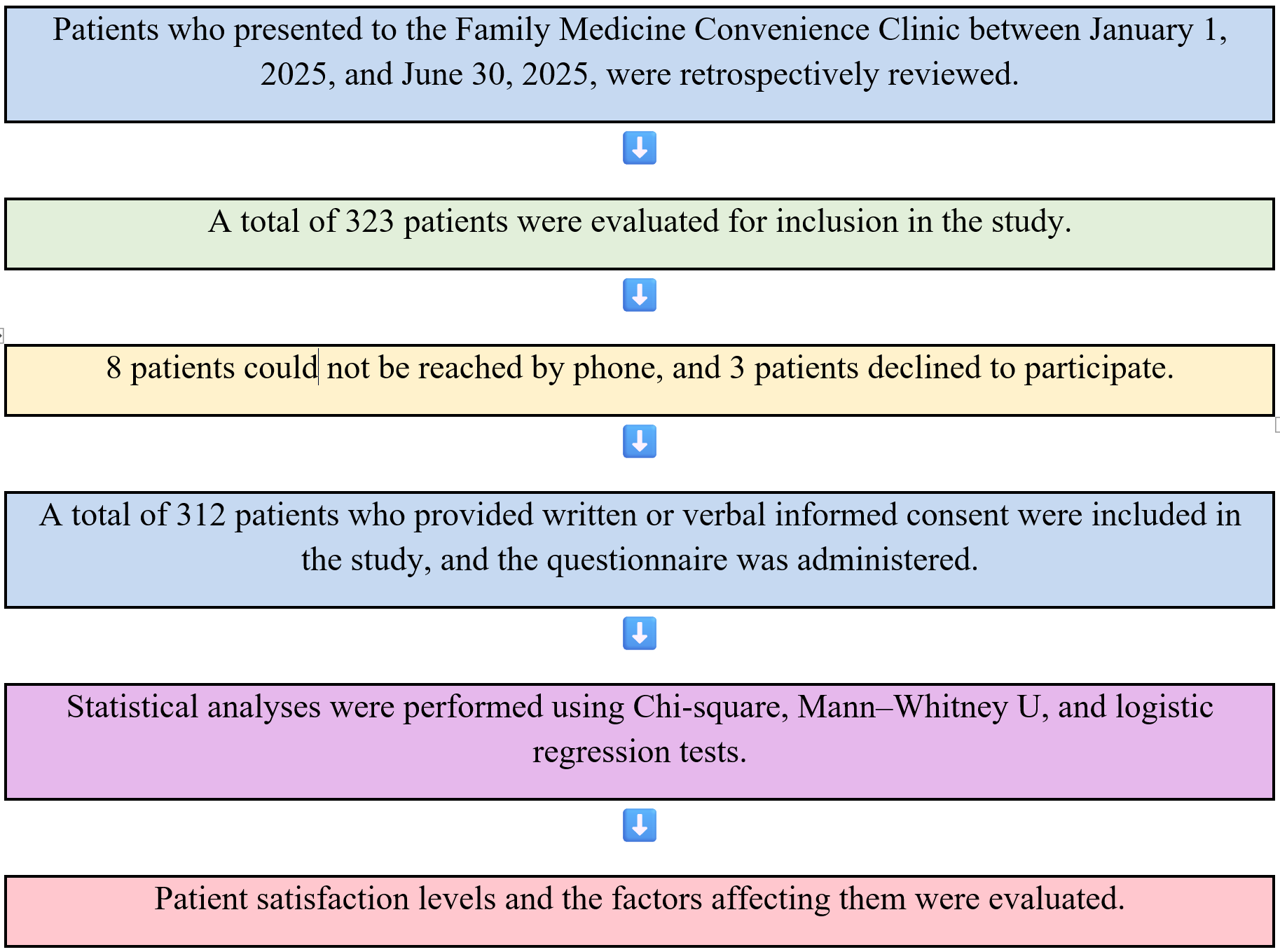
Using the G*Power 3.1 program for sample size analysis, it was calculated that at least 250 participants should be included in the study under the assumptions of 80% power (1-β=0.80), 5% significance level (α=0.05), and a medium effect size. Considering possible data loss and non-participation, the target sample size was planned to be 350 individuals. A total of 323 patients who visited the outpatient clinic during the specified time period were evaluated; after excluding individuals who could not be reached or who refused to participate, 312 patients were included in the study, and the analyses were performed on this sample (Figure 1)
Data collection process
Data were collected from clinical information obtained through the hospital information management system and a questionnaire form prepared by the researchers in accordance with the literature. The questionnaire consists of two sections:
- The first section comprises questions assessing sociodemographic (age, gender, education level, marital status, presence of chronic disease, etc.) and clinical characteristics.
- The second section includes the Patient Satisfaction Assessment Short Form (PSASF).
Patient satisfaction was measured using the 7-item, 5-point Likert-type PSASF. The total score of the scale ranges from 0 to 28, with higher scores indicating greater levels of dissatisfaction. The sixth item of the scale is reverse-coded. According to the original classification, scores of 0–10 are rated as “very satisfied,” 11–18 as “satisfied,” 19–26 as “dissatisfied,” and 27–28 as “very dissatisfied.”
The PSASF was developed by Hawthorne et al.[11] and adapted into Turkish by Temeloğlu Şen and Sertel Berk.[12] It has been reported that the scale has a single-factor structure and an internal consistency coefficient of Cronbach's alpha = .87.
In this study, due to the low number of patients in subgroups, the scoring was reclassified into two categories: 0–18 as “satisfied” and >18 as “dissatisfied.” The questionnaire was administered either face-to-face or by telephone based on participant preference; the same standardized form was used in both methods.
Statistical analysis
Statistical analysis of the data was performed using IBM SPSS Statistics for Windows, Version 22.0 (IBM Corp., Armonk, NY, USA). The distribution of continuous variables was assessed with the Kolmogorov–Smirnov test; data not following a normal distribution were presented as median (minimum–maximum). Categorical variables were expressed as frequency (percentage). For intergroup comparisons, the chi-square test or Fisher’s exact test (when appropriate) was used for categorical variables, and the Mann–Whitney U test was used for continuous variables. Statistical significance was accepted at p<0.05 in all analyses.
Results
The median age of the 312 patients included in the study was 45 (min: 0, max: 70). Of the participants, 79.8% were female and 20.2% were male. Regarding educational attainment, the highest proportion was observed among university graduates (40.7%). At least one chronic disease was present in 44.2% of the patients. Examination of the reasons for presentation revealed that 76.6% of the patients presented to the convenience polyclinic for radiological examinations, while 23.4% applied for laboratory tests. The demographic and clinical characteristics of the participants are summarized in Table 1.
| Table 1. Demographic and clinical characteristics of patients admitted to the family medicine convenience clinic (n = 312) | ||
| Variable |
|
|
| Age (years) |
(Min = 0, Max = 70) |
|
| Gender | ||
| Female |
|
|
| Male |
|
|
| Education level | ||
| Primary school |
|
|
| High school |
|
|
| University |
|
|
| Accompanying illness | ||
| Yes |
|
|
| No |
|
|
| Reason for application | ||
| Radiology examination |
|
|
| Laboratory examination |
|
|
When satisfaction levels of patients presenting to the polyclinic were evaluated, 59.6% reported being very satisfied with treatment or care outcomes, 62.5% with explanations provided by physicians or other healthcare professionals, 62.2% with attentive behavior during the examination process, and 60.3% with their involvement in health-related decisions. A total of 66.0% of patients indicated being very satisfied with the respectful attitude of healthcare personnel, representing the highest level of satisfaction. The lowest satisfaction rate, at 33.0%, was reported regarding the time spent with the physician. The detailed distribution of these findings is presented in Table 2.
| Table 2. Patient satisfaction levels according to the short form of patient satisfaction evaluation (n, %) | |||||
| Survey Question |
|
|
n (%) |
|
|
| How satisfied are you with the treatment or care outcomes? |
|
|
|
|
|
| How satisfied are you with the explanations provided by the doctor or other healthcare professional regarding the treatment/care outcomes? |
|
|
|
|
|
| How attentive was the doctor or other healthcare professional during the examination? |
|
|
|
|
|
| How satisfied are you with your level of participation in decisions regarding the healthcare you received? |
|
|
|
|
|
| How satisfied are you with the respect shown to you by the doctor or other healthcare professional? |
|
|
|
|
|
| Do you find the time spent with the doctor sufficient? |
|
|
|
|
|
| How satisfied are you with the general care shown to you at the hospital or clinic? |
|
|
|
|
|
Examination of parameters reflecting patient satisfaction revealed an overall satisfaction rate of 92.6% (n = 289). When stratified by age group, the satisfaction level among individuals in the advanced age group (98.7%) was significantly higher compared to the younger age group (p < 0.001). Furthermore, statistically significant associations were identified between satisfaction level and female gender (p = 0.019), lower education level (p = 0.050), and the presence of chronic disease (p = 0.024). Accordingly, satisfaction rates were higher among female patients, those with lower educational attainment, and individuals with chronic conditions. In contrast, no significant difference was observed between the reason for application (radiological or laboratory examination) and satisfaction level (p = 0.064) (Table 3).
| Note: Data are presented as numbers (percentages). Differences between groups were assessed using the chi-square test or Fisher's exact test. p< 0.05 was considered statistically significant. | |||
| Table 3. Relationship between patient satisfaction level and demographic and clinical characteristics | |||
| Variable |
n (%) |
n (%) |
|
| Age group (Median 45) |
|
||
| Young age (<45) |
|
|
|
| Old age (≥45) |
|
|
|
| Gender |
|
||
| Female |
|
|
|
| Male |
|
|
|
| Education level |
|
||
| Primary school and below |
|
|
|
| Middle school |
|
|
|
| High school |
|
|
|
| University and above |
|
|
|
| Comorbidities |
|
||
| Present |
|
|
|
| Absent |
|
|
|
| Reason for referral |
|
||
| Radiology examination |
|
|
|
| Laboratory examination |
|
|
|
Factors associated with patient satisfaction among patients visiting the Convenience Clinic were initially examined using univariate logistic regression analysis. In the univariate analysis, age (p=0.001), gender (p=0.023), education level (overall p=0.052), comorbidities (p=0.031), and reason for visit (p=0.070) were found to be statistically related to patient satisfaction. Variables showing significance at the p<0.10 level in univariate analysis were included in the multivariate logistic regression model. Multivariate analysis revealed that only the age variable remained independently associated with patient satisfaction (OR=9.77; 95% CI: 1.80–53.06; p=0.008). The variables of gender (p=0.684), education level (overall p=0.442), presence of comorbidities (p=0.595), and reason for referral (p=0.919) lost their statistical significance in the multivariate model (Table 4).
|
Reference categories: Age <45 years, Female gender, Primary education, Presence of comorbidity. OR: Odds Ratio; CI: Confidence Interval. |
||||
| Table 4. Univariable and multivariable logistic regression analysis of factors associated with patient satisfaction | ||||
| Variable |
|
|
|
|
| Age ≥45 (vs <45) |
|
|
|
|
| Male (vs Female) |
|
|
|
|
| Education (overall) |
|
|
|
|
| High school (vs Primary) |
|
|
|
|
| University (vs Primary) |
|
|
|
|
| No comorbidity (vs Yes) |
|
|
|
|
Discussion
This study evaluated the real-world effects of digital integration between primary healthcare services and hospital services. The patient satisfaction evaluated in this study reflects the perception of the services provided within the scope of the Family Medicine Convenience Clinic and covers the participants' experiences regarding the examination approval and referral process they received through the clinic. In this context, the findings obtained should not be directly compared with satisfaction levels regarding general hospital services or other clinics and should only be interpreted within the framework of the Convenience Clinic application. The Convenience Polyclinic model has been shown to facilitate access to healthcare services, improve the patient experience, and increase overall satisfaction levels.
This study evaluated only individuals who received services from the Family Medicine Convenience Clinic; no comparative analysis was conducted with individuals who did not receive services. Therefore, the findings do not include comparative conclusions and should be interpreted within the context of the impact of the Convenience Clinic program on patient satisfaction.
Review of the literature indicates that the primary factors influencing patient satisfaction are the quality of medical care, physician-patient communication, and waiting time. It has been emphasized that waiting time is particularly critical for satisfaction; while short durations may go unnoticed, prolonged waiting significantly increases dissatisfaction. The same studies report that age, education level, and perceived health status also affect satisfaction, with older individuals and those with lower educational attainment generally exhibiting higher satisfaction.[13-15]
Previous studies demonstrated that satisfaction in primary healthcare services is generally high, with communication quality, respect, and privacy being among the most satisfying aspects; however, appointment scheduling and waiting times negatively impact satisfaction.[16] These findings from the literature were also observed in our study. The overall satisfaction rate obtained in our study was higher than those reported in both referenced studies. Higher satisfaction levels among females, older adults, and individuals with lower education levels support the influence of sociodemographic characteristics on satisfaction. This may be explained by the relatively lower expectations of healthcare services among older and less-educated individuals, as well as their more frequent contact with healthcare facilities. Studies evaluating the effectiveness of family medicine have reported that strengthening primary healthcare services reduces unnecessary hospital visits and enhances efficiency within the healthcare system.[17-19] In our study, the majority of patients applied for examination approval, enabling them to complete their procedures without directly visiting hospital outpatient clinics. Although examinations in the Convenience Polyclinic are conducted within the hospital, patients are directed to the relevant units without requiring a separate consultation appointment or prolonged waiting. This structure allows patients to access radiology or laboratory units solely through the examination approval process, thereby preventing time loss and reducing hospital congestion. In this regard, the system, even in its current form, provides significant convenience and increased satisfaction in healthcare delivery. Hedayatipour et al. stated that evidence-based administrative decision-making processes enhance the efficiency, equity, and sustainability of healthcare services; however, limitations in time, resources, and access to information may restrict these processes.[5] In the Convenience Polyclinic model, the provision of digital integration contributes to overcoming such structural limitations, enabling process acceleration and the applicability of data-driven decisions. Another study reported that delays in the follow-up of abnormal mammography results at the primary care level are primarily due to communication deficiencies and inadequate coordination. In the Convenience Polyclinic model, digital integration allows direct access to examination results, thereby minimizing such communication delays and strengthening service continuity. Previous studies identified communication quality, waiting time, and ease of access as the strongest determinants of patient satisfaction.[15] In our study, it was observed that these three factors were simultaneously improved within the Convenience Polyclinic model. This finding explains the high overall satisfaction rates and is consistent with studies in the literature. In particular, short wait times and ease of referral have positively influenced the patient experience. The international literature has shown that the public financing and social protection-based approach of the Seguro Popular system implemented in Mexico has reduced catastrophic out-of-pocket expenditures and decreased inequalities in access to services.[20] Similarly, it has been reported that progress toward universal health coverage has reduced infant, child, and maternal mortality rates, and that public financing and system integration have played a decisive role in this process.[21] The high satisfaction rate obtained in our study indicates that digital integration practices in Türkiye, particularly through the Convenience Polyclinic model, strengthen coordination between primary care and hospital services and reduce access inequalities.
The digital integration program implemented by the Turkish Ministry of Health also covers referral processes from family health centers to hospitals. Thanks to this system, individuals assessed at the primary care level can be referred to hospital services in a more organized and efficient manner. It is believed that the Convenience Clinic model plays an important bridging role within this digital integration structure and positively impacts the service access experience of individuals seeking care. Our study has certain limitations. It should be noted that some individuals who apply to the Convenience Clinic may be healthy individuals without active disease complaints who are applying for screening or examination approval. As the research was conducted at a single center over a six-month period (January 1, 2025–June 30, 2025), the results may not fully reflect seasonal variations and have limited generalizability. Additionally, due to the low number of specific imaging procedures such as ultrasonography and radiography, imaging examinations were grouped under a single category, which restricted the analysis of differences between subgroups. The cross-sectional design is inadequate for establishing causality, and self-reported data on patient satisfaction may be influenced by subjective response biases. Furthermore, Patient Satisfaction Assessment Short Form (PSASF) scores were dichotomized into 0–18 as “satisfied” and >18 as “dissatisfied” due to the low number of patients in subgroups, which may have partially reduced the sensitivity of the scale. This study is pioneering and original, as it represents the first evaluation of Convenience Polyclinic practices in Türkiye from the perspective of patient satisfaction.
Conclusion
In conclusion, the “Convenience Polyclinic” model stands out as an innovative application that, in alignment with digital transformation policies, enhances accessibility and efficiency in healthcare services while strengthening patient satisfaction. This model optimizes referral and referral processes by creating functional integration between primary care and hospital services; it is thought that this could contribute to reducing unnecessary tertiary care referrals. The findings indicate that expanding digital integration could make significant contributions to universal inclusivity and service quality in primary healthcare services in Türkiye.
Ethical approval
This study was approved by the Ethics Committee of Gülhane Training and Research Hospital (Approval date: May 08, 2025; Decision No: 2025/97).
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest to disclose.
Referanslar
- World Health Organization (WHO). Primary health care: transforming vision into action. Geneva: WHO; 2018.
- Meunier PY, Raynaud C, Guimaraes E, Gueyffier F, Letrilliart L. Barriers and facilitators to the use of clinical decision support systems in primary care: a mixed-methods systematic review. Ann Fam Med. 2023;21(1):57-69. https://doi.org/10.1370/afm.2908
- Republic of Turkey Ministry of Health. Health transformation program in Turkey: progress report, January 2009. Ankara: Ministry of Health; 2009.
- Ferreira DC, Vieira I, Pedro MI, Caldas P, Varela M. Patient satisfaction with healthcare services and the techniques used for its assessment: a systematic literature review and a bibliometric analysis. Healthcare (Basel). 2023;11(5):639. https://doi.org/10.3390/healthcare11050639
- Hedayatipour M, Etemadi S, Hekmat SN, Moosavi A. Challenges of using evidence in managerial decision-making of the primary health care system. BMC Health Serv Res. 2024;24(1):38. https://doi.org/10.1186/s12913-023-10409-7
- Ohta R, Sano C. The Effectiveness of family medicine-driven interprofessional collaboration on the readmission rate of older patients. Healthcare (Basel). 2023;11(2):269. https://doi.org/10.3390/healthcare11020269
- Greenwood-Lee J, Jewett L, Woodhouse L, Marshall DA. A categorisation of problems and solutions to improve patient referrals from primary to specialty care. BMC Health Serv Res. 2018;18(1):986. https://doi.org/10.1186/s12913-018-3745-y
- Republic of Türkiye Ministry of Health, General Directorate of Public Health. Integration between levels of healthcare services. Ankara: Republic of Türkiye Ministry of Health; 2024. Available at: https://hsgm.saglik.gov.tr/depo/Mevzuat/Genel_Nitelikli_Yazi_ve_Gorusler/Saglik_Basamaklari_Arasinda_Entegrasyon.pdf (Accessed on Jun 18, 2026).
- Reece JC, Neal EFG, Nguyen P, McIntosh JG, Emery JD. Delayed or failure to follow-up abnormal breast cancer screening mammograms in primary care: a systematic review. BMC Cancer. 2021;21(1):373. https://doi.org/10.1186/s12885-021-08100-3
- Bolton Saghdaoui L, Lampridou S, Tavares S, et al. Interventions to improve referrals from primary care to outpatient specialist services for chronic conditions: a systematic review and framework synthesis update. Syst Rev. 2025;14(1):103. https://doi.org/10.1186/s13643-025-02841-z
- Hawthorne G, Sansoni J, Hayes L, Marosszeky N, Sansoni E. Measuring patient satisfaction with health care treatment using the short assessment of patient satisfaction measure delivered superior and robust satisfaction estimates. J Clin Epidemiol. 2014;67(5):527-537. https://doi.org/10.1016/j.jclinepi.2013.12.010
- Temeloğlu Şen E, Sertel Berk HÖ. Hasta Memnuniyeti Kısa Değerlendirme Formu'nun (HMKDF) Türkçe uyarlama çalışması. İstanbul Ticaret Üniversitesi Sosyal Bilimler Dergisi. 2022;21(43):35-54. https://doi.org/10.46928/iticusbe.880433
- Öztürk SC, Avcı K. An investigation of patient experiences from outpatient to inpatient services in an integrated health campus: the case of Ankara Etlik City Hospital. Anatol J Gen Med Res. 2025;35:159-169. https://doi.org/10.4274/anatoljmed.2025.42713
- Alrasheedi KF, Al-Mohaithef M, Edrees HH, Chandramohan S. The association between wait times and patient satisfaction: findings from primary health centers in the kingdom of saudi arabia. Health Serv Res Manag Epidemiol. 2019;6:2333392819861246. https://doi.org/10.1177/2333392819861246
- Xiao H, Barber JP. The effect of perceived health status on patient satisfaction. Value Health. 2008;11(4):719-725. https://doi.org/10.1111/j.1524-4733.2007.00294.x
- Harutyunyan T, Demirchyan A, Thompson ME, Petrosyan V. Patient satisfaction with primary care in Armenia: good rating of bad services? Health Serv Manage Res. 2010;23(1):12-17. https://doi.org/10.1258/hsmr.2009.009012
- Carai S, Park M, Schurmann A, Breda J, Azzopardi-Muscat N, Weber M. The impact of primary health care on efficiency and quality of care. In: Rajan D, Rouleau K, Winkelmann J, et al., editors. Implementing the primary health care approach: a primer. Copenhagen: European Observatory on Health Systems and Policies; 2024.
- Sánchez-Piedra CA, Prado-Galbarro FJ, García-Pérez S, Santamera AS. Factors associated with patient satisfaction with primary care in Europe: results from the EUprimecare project. Qual Prim Care. 2014;22(3):147-155.
- Kringos DS, Boerma W, van der Zee J, Groenewegen P. Europe's strong primary care systems are linked to better population health but also to higher health spending. Health Aff (Millwood). 2013;32(4):686-694. https://doi.org/10.1377/hlthaff.2012.1242
- Knaul FM, González-Pier E, Gómez-Dantés O, et al. The quest for universal health coverage: achieving social protection for all in Mexico. Lancet. 2012;380(9849):1259-1279. https://doi.org/10.1016/S0140-6736(12)61068-X
- Moreno-Serra R, Smith PC. Does progress towards universal health coverage improve population health? Lancet. 2012;380(9845):917-923. https://doi.org/10.1016/S0140-6736(12)61039-3
Telif hakkı ve lisans
Telif Hakkı © 2026 Yazar(lar). Açık erişimli bu makale, orijinal çalışmaya uygun şekilde atıfta bulunulması koşuluyla, herhangi bir ortamda veya formatta sınırsız kullanım, dağıtım ve çoğaltmaya izin veren Creative Commons Attribution License (CC BY) altında dağıtılmıştır.